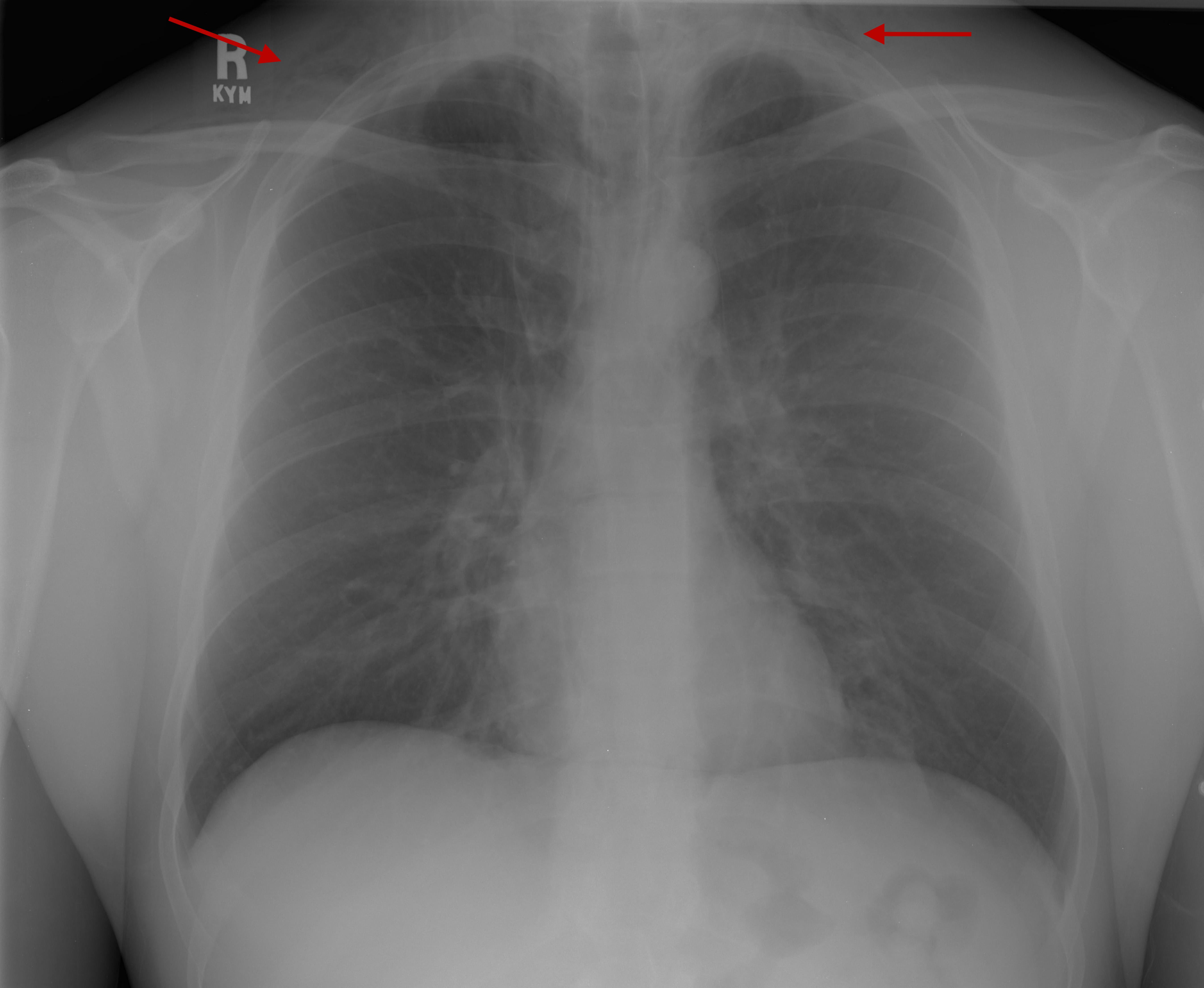
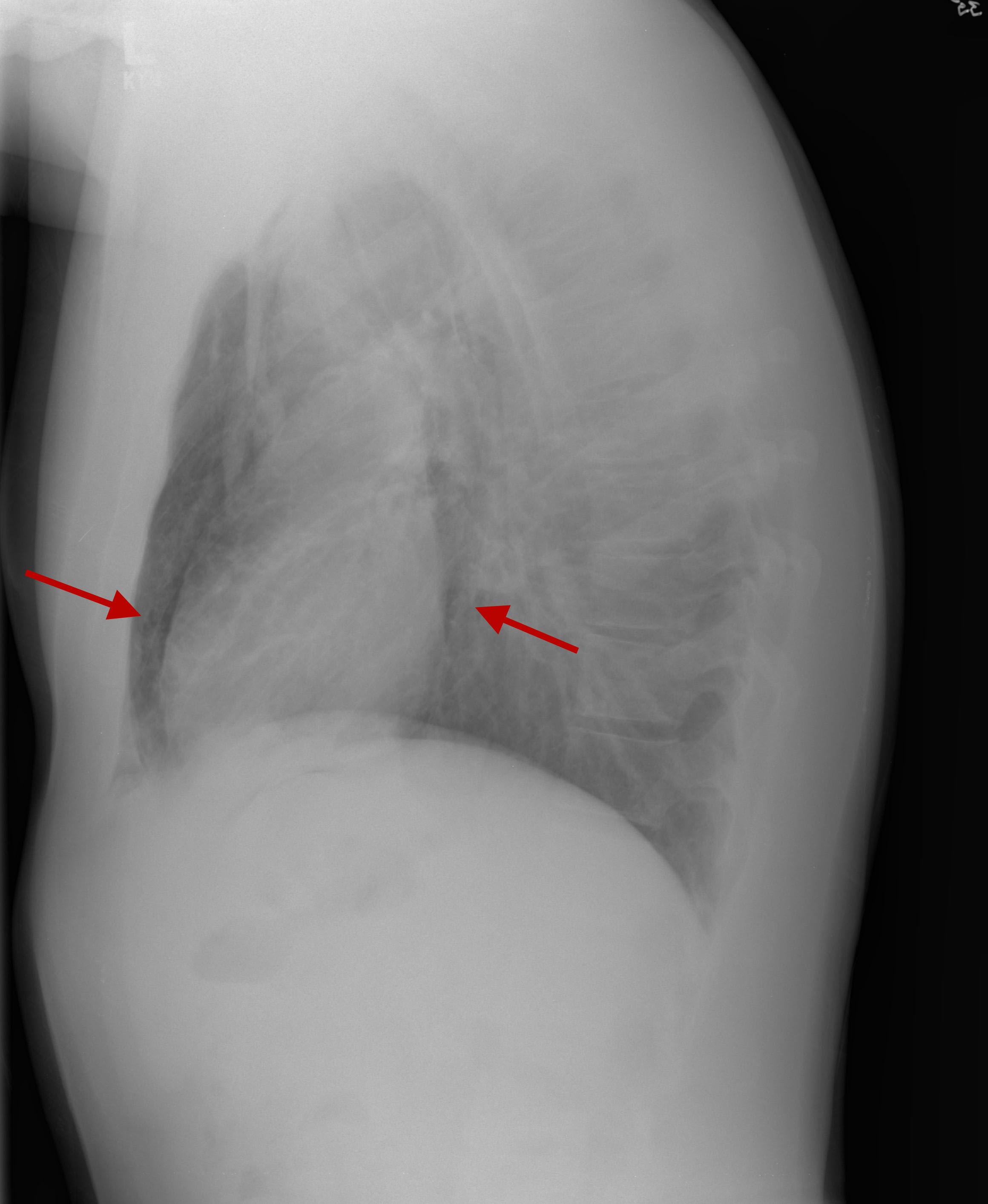
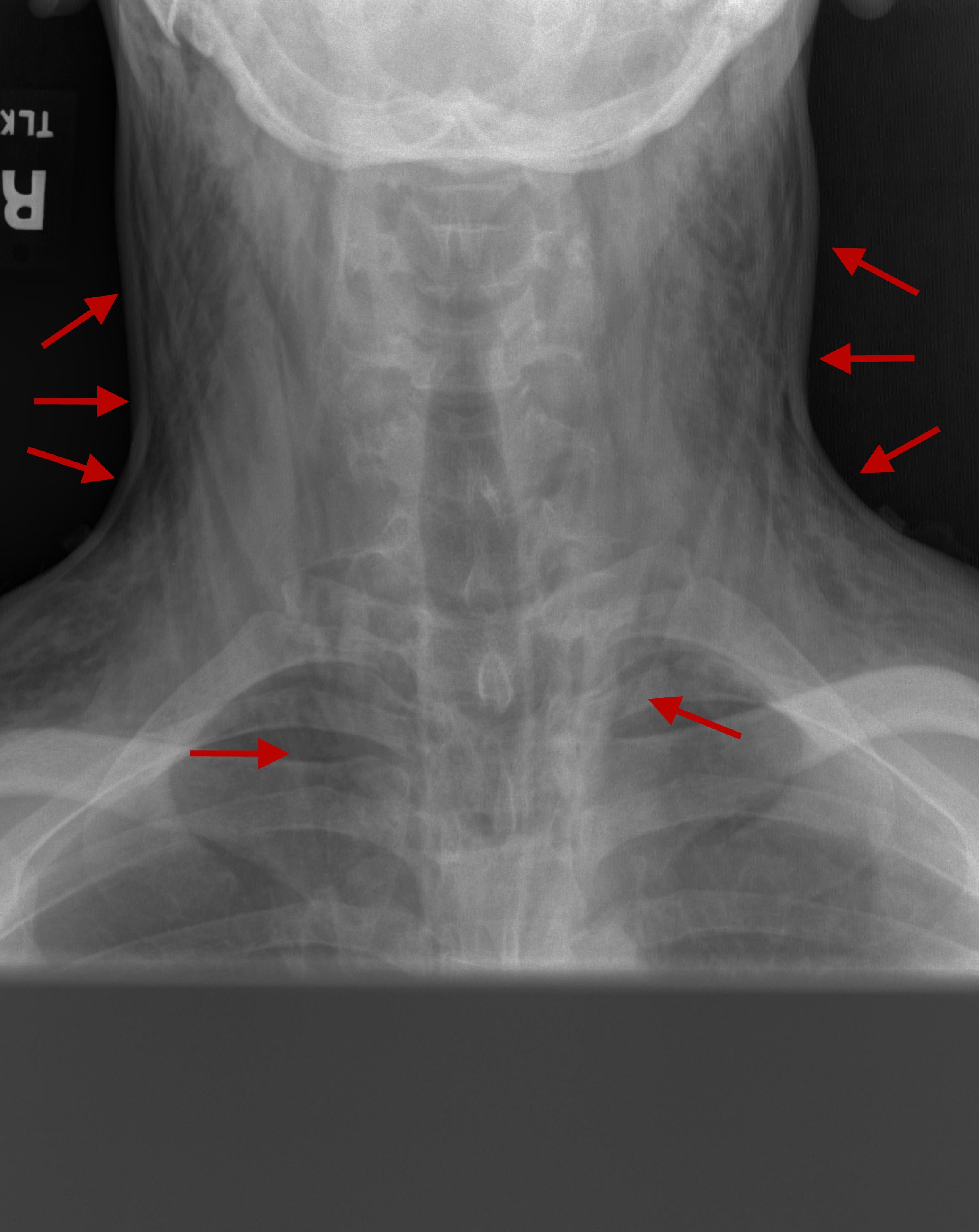
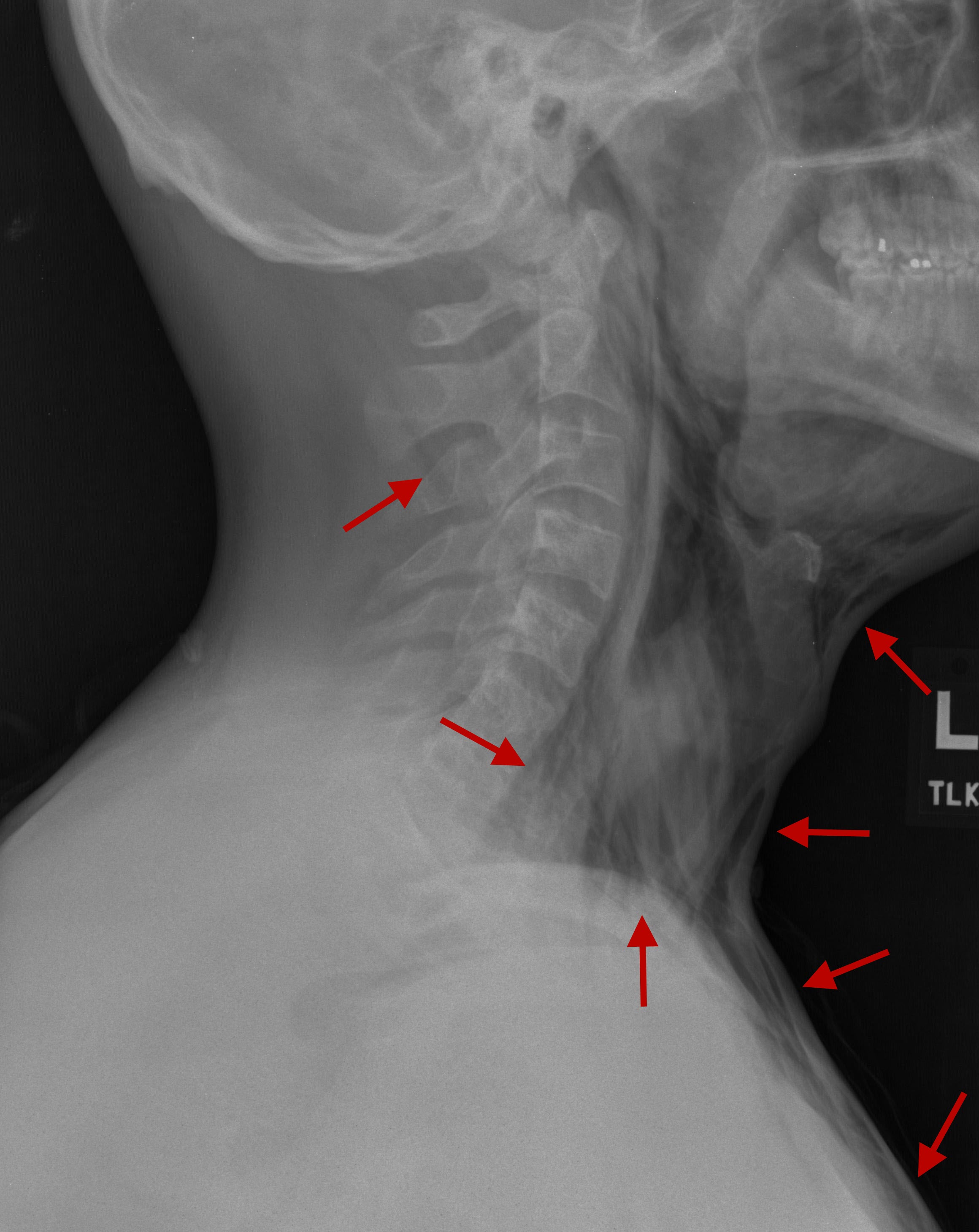
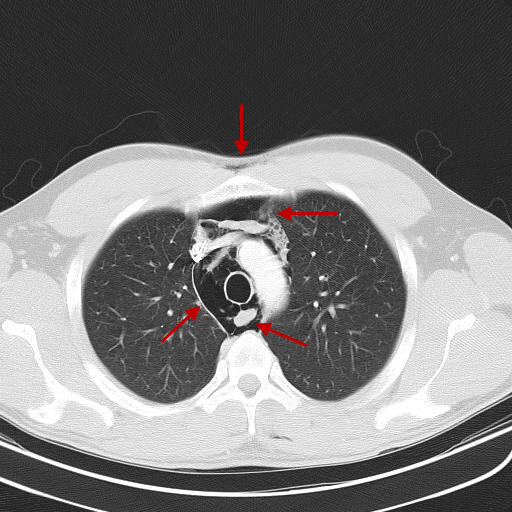
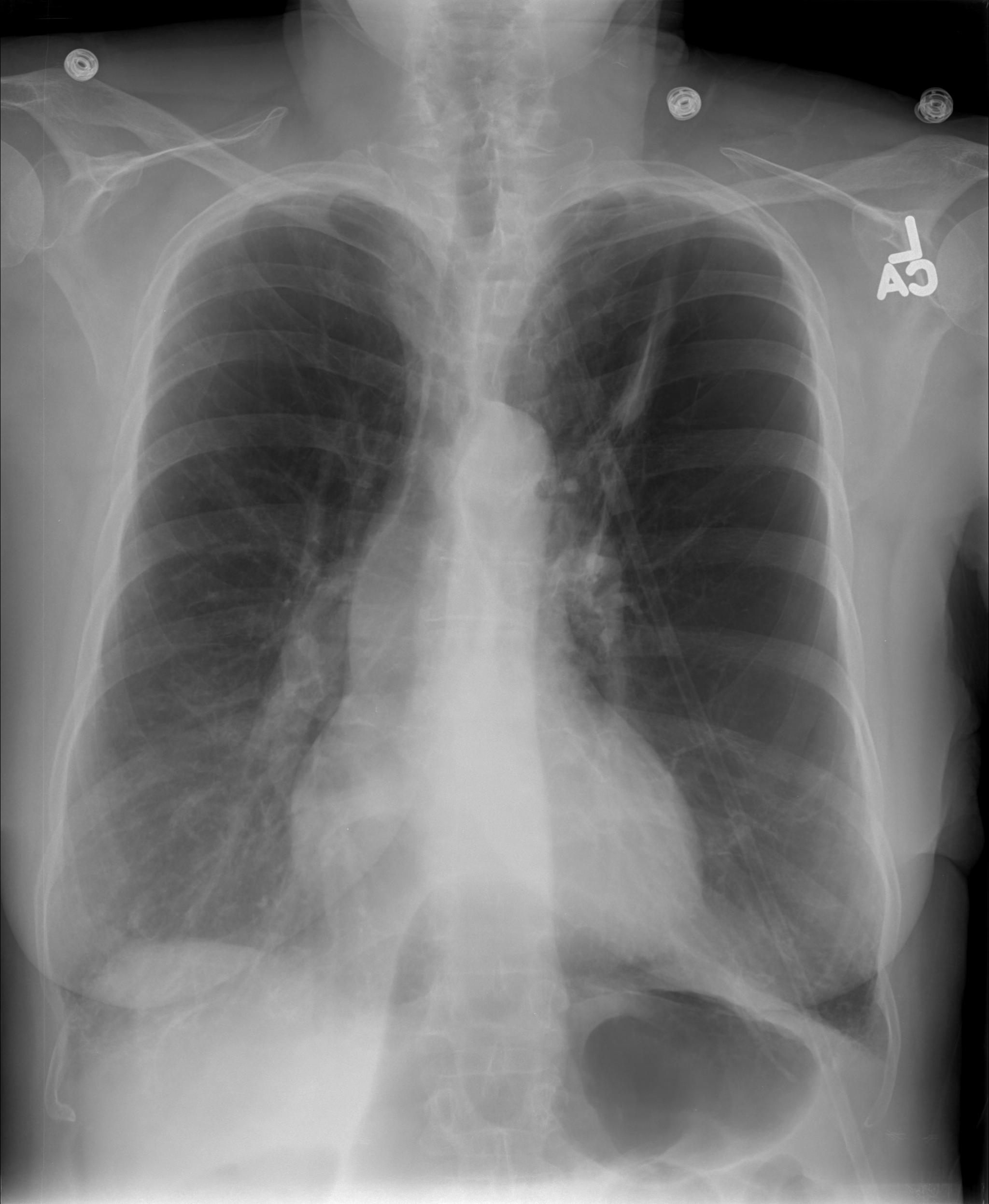
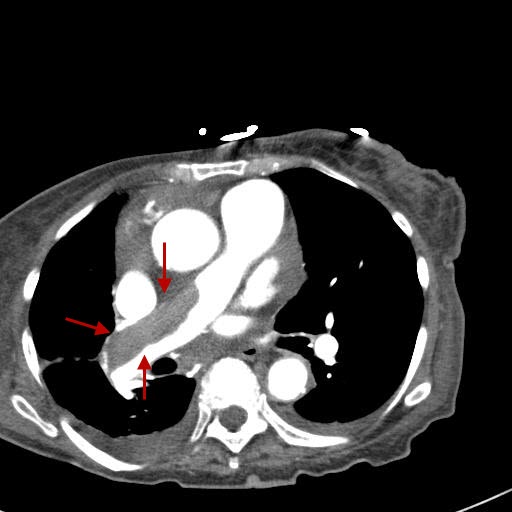
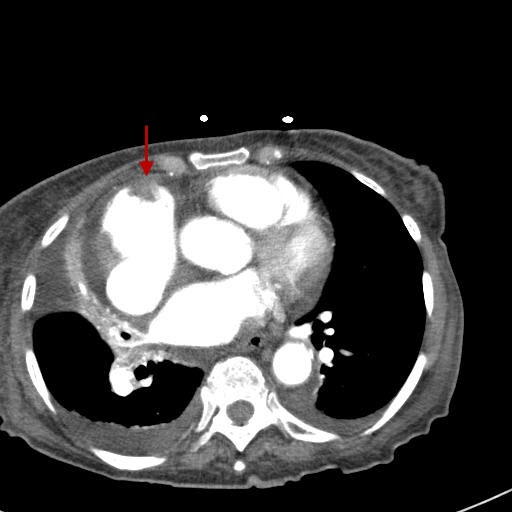
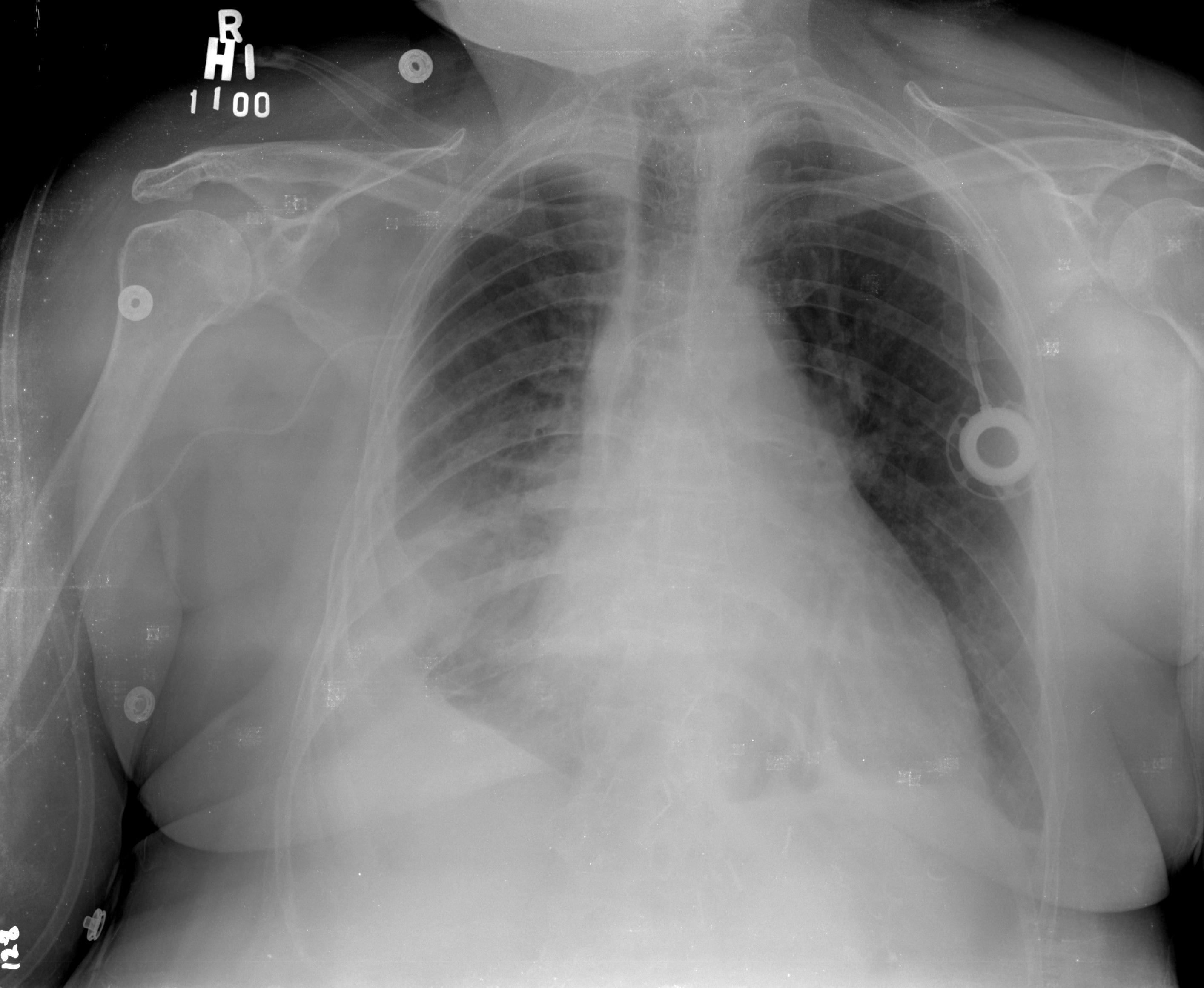
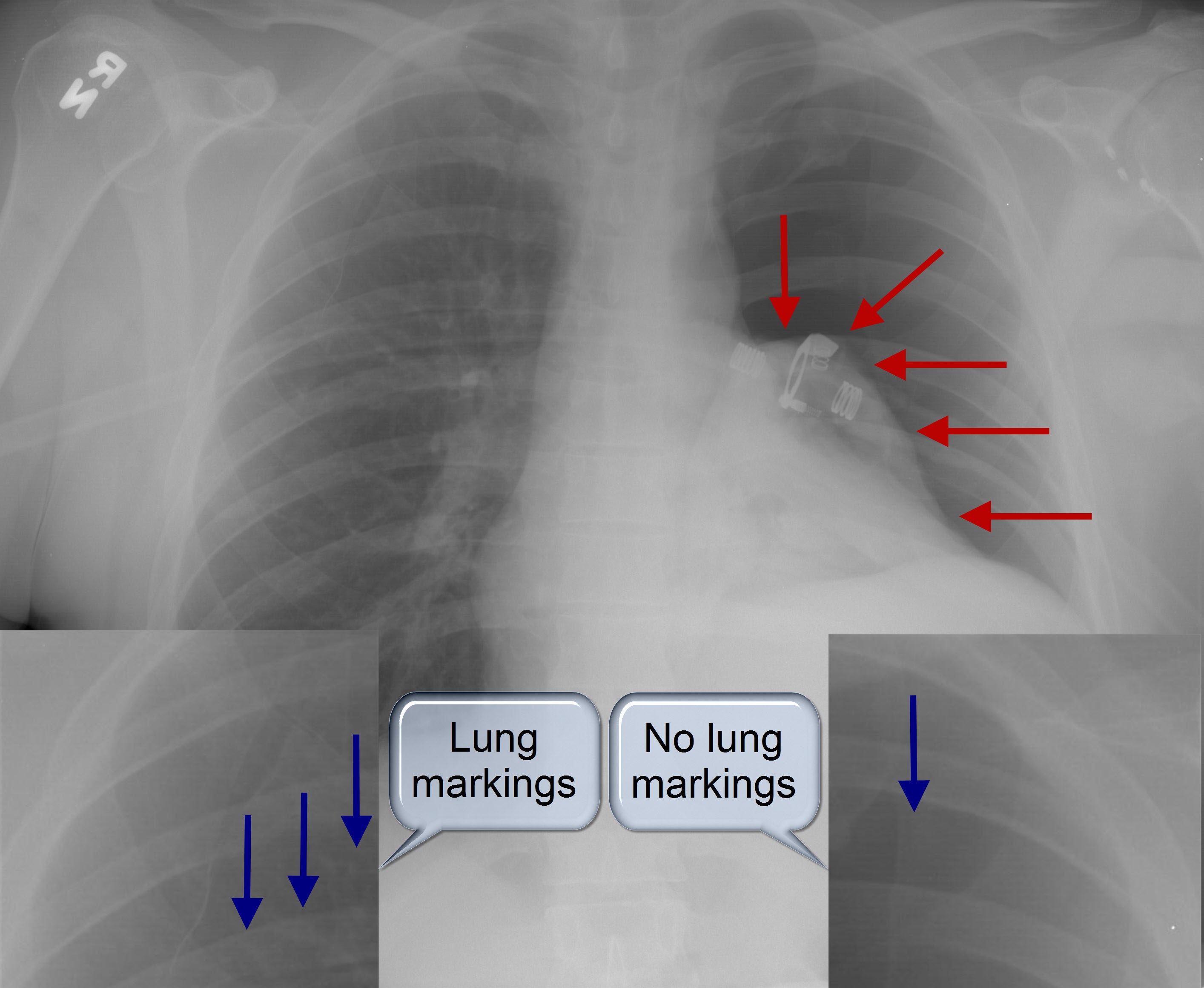
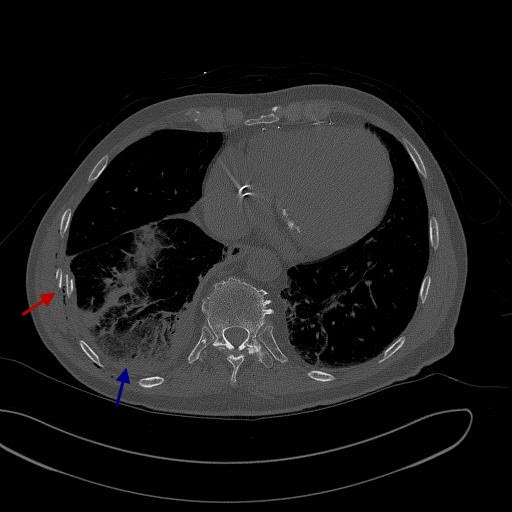
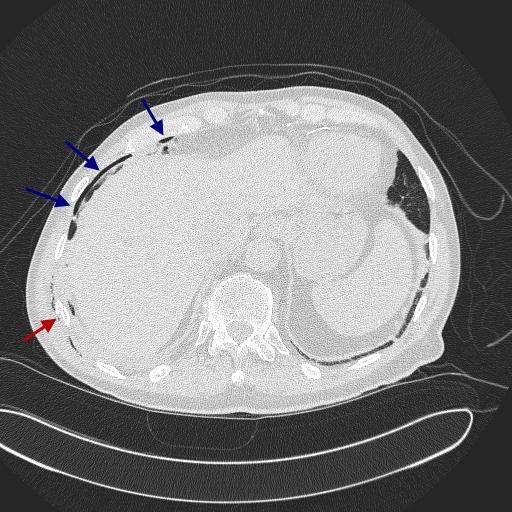
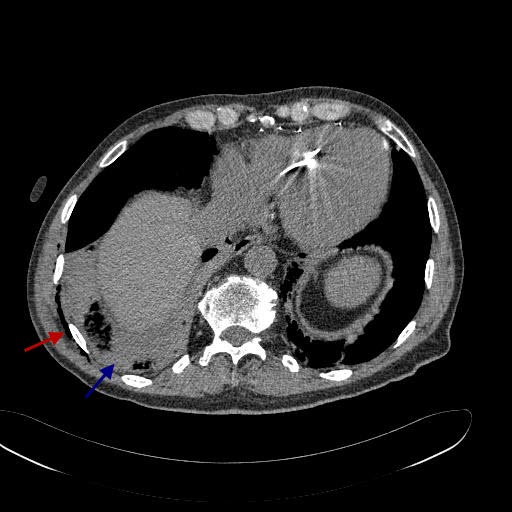
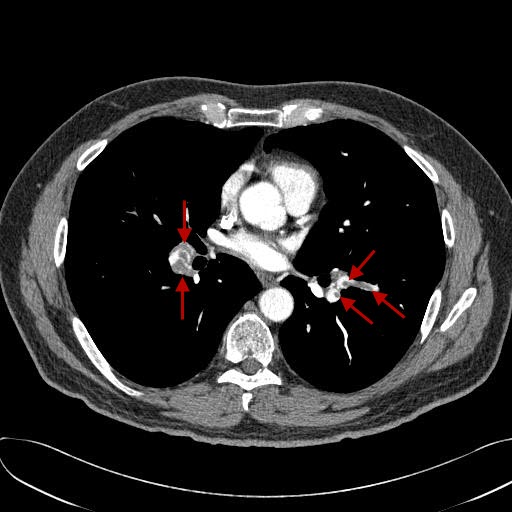
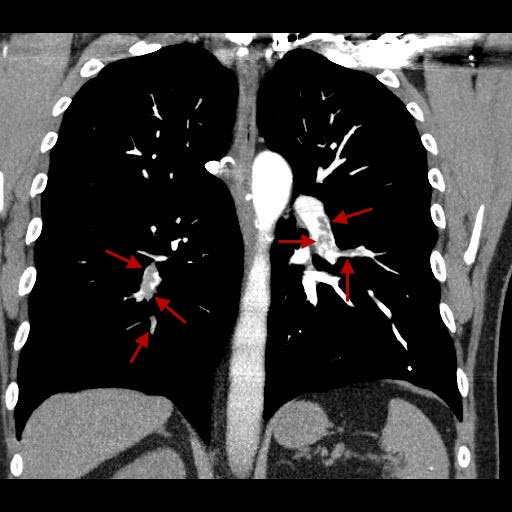
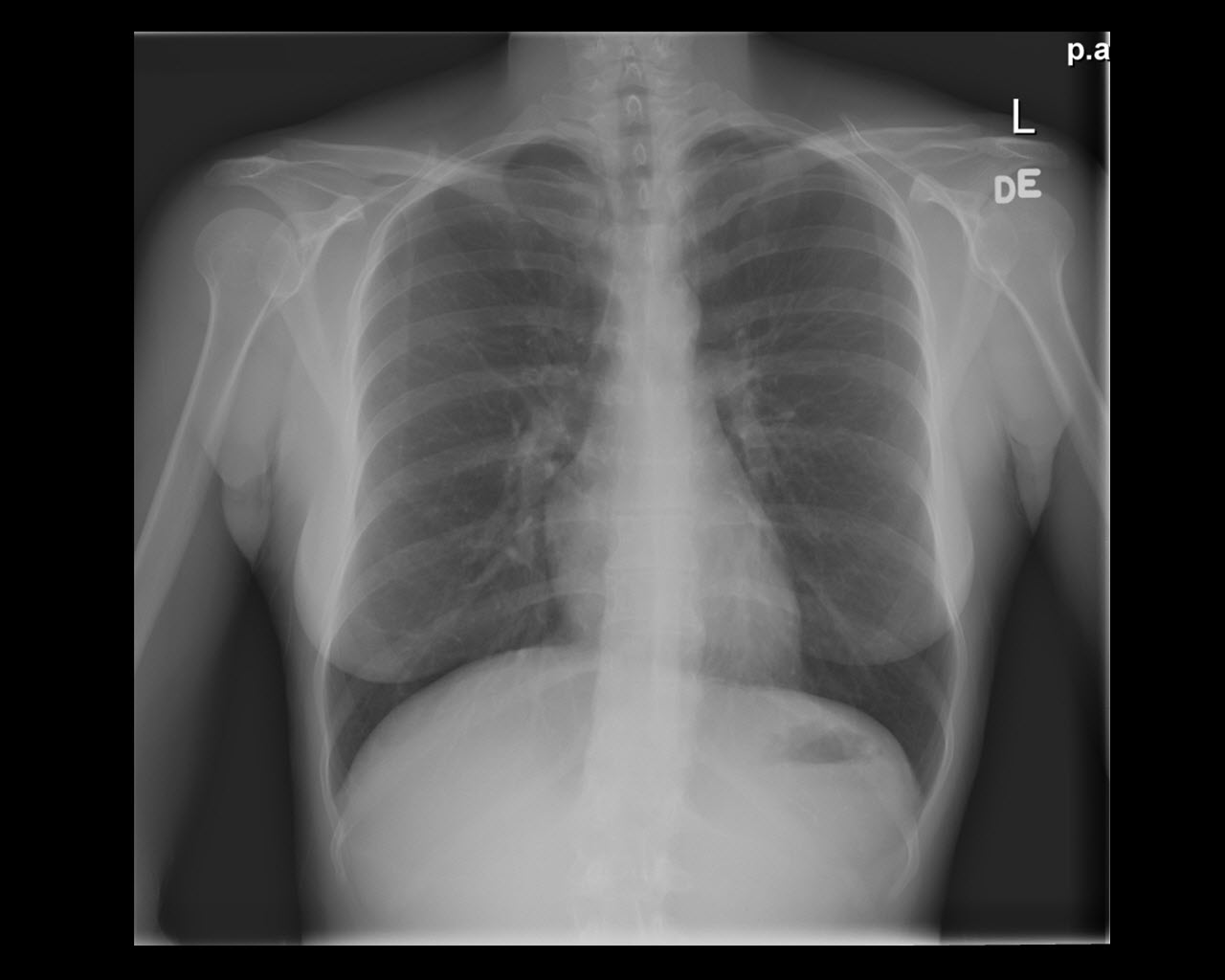
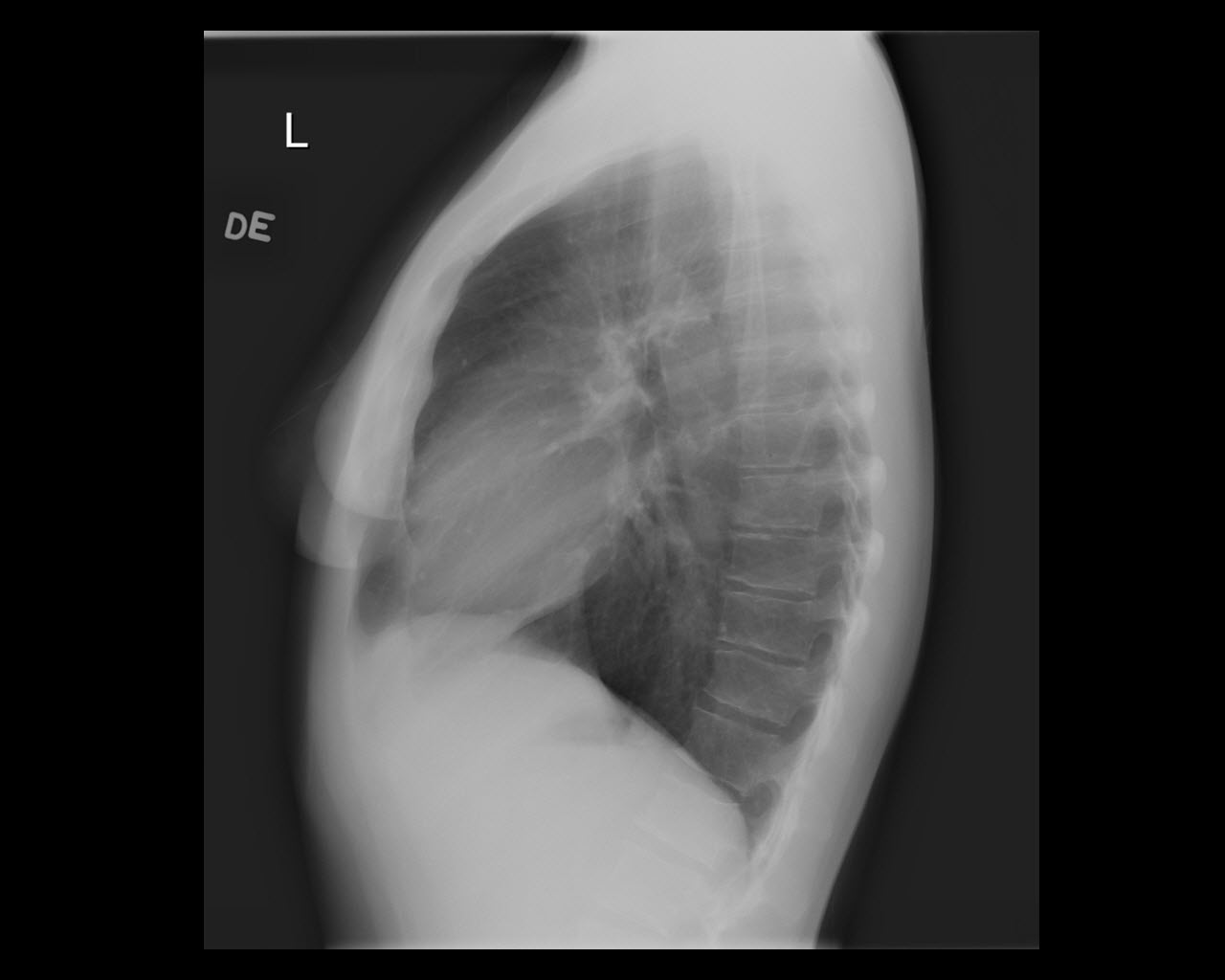
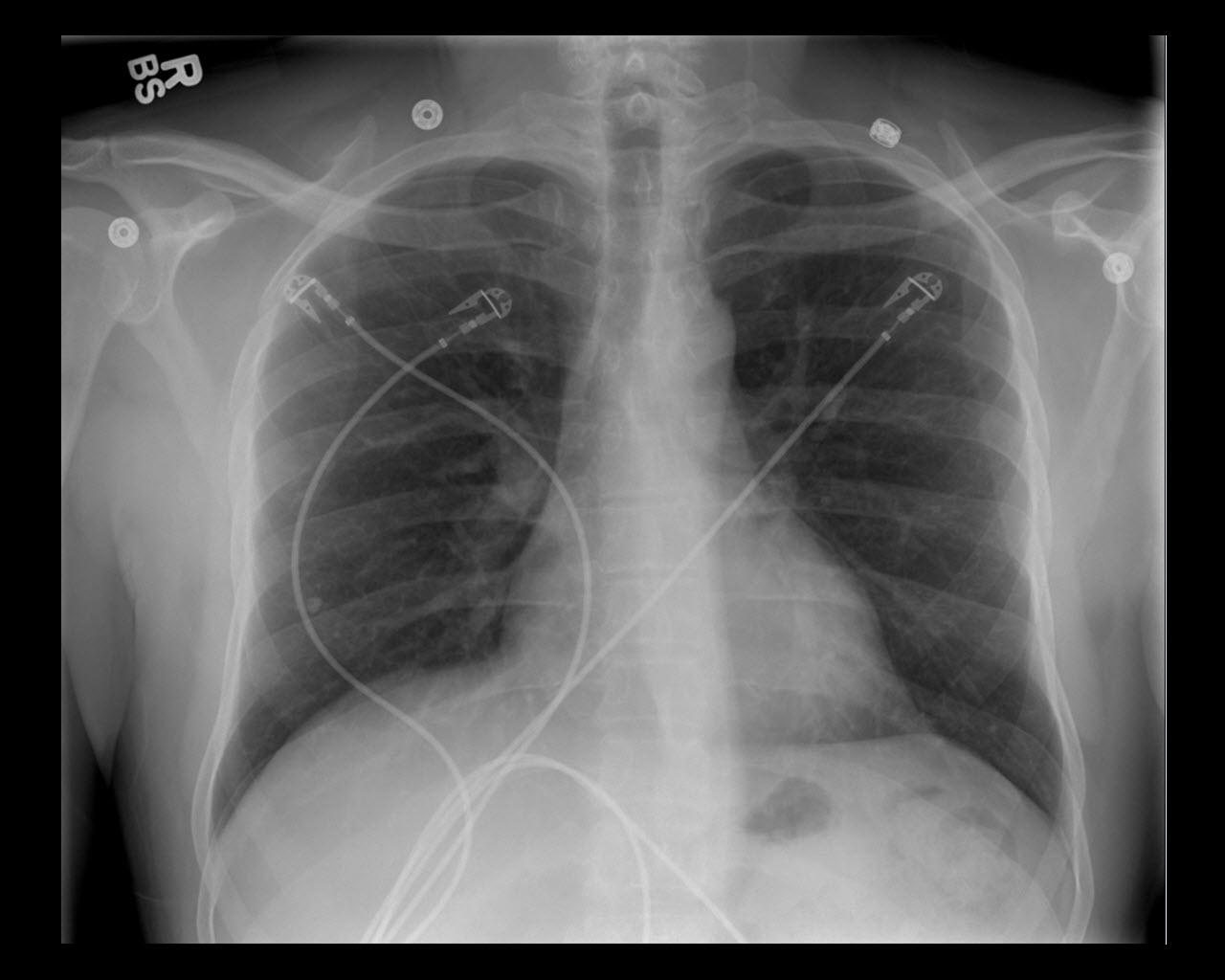
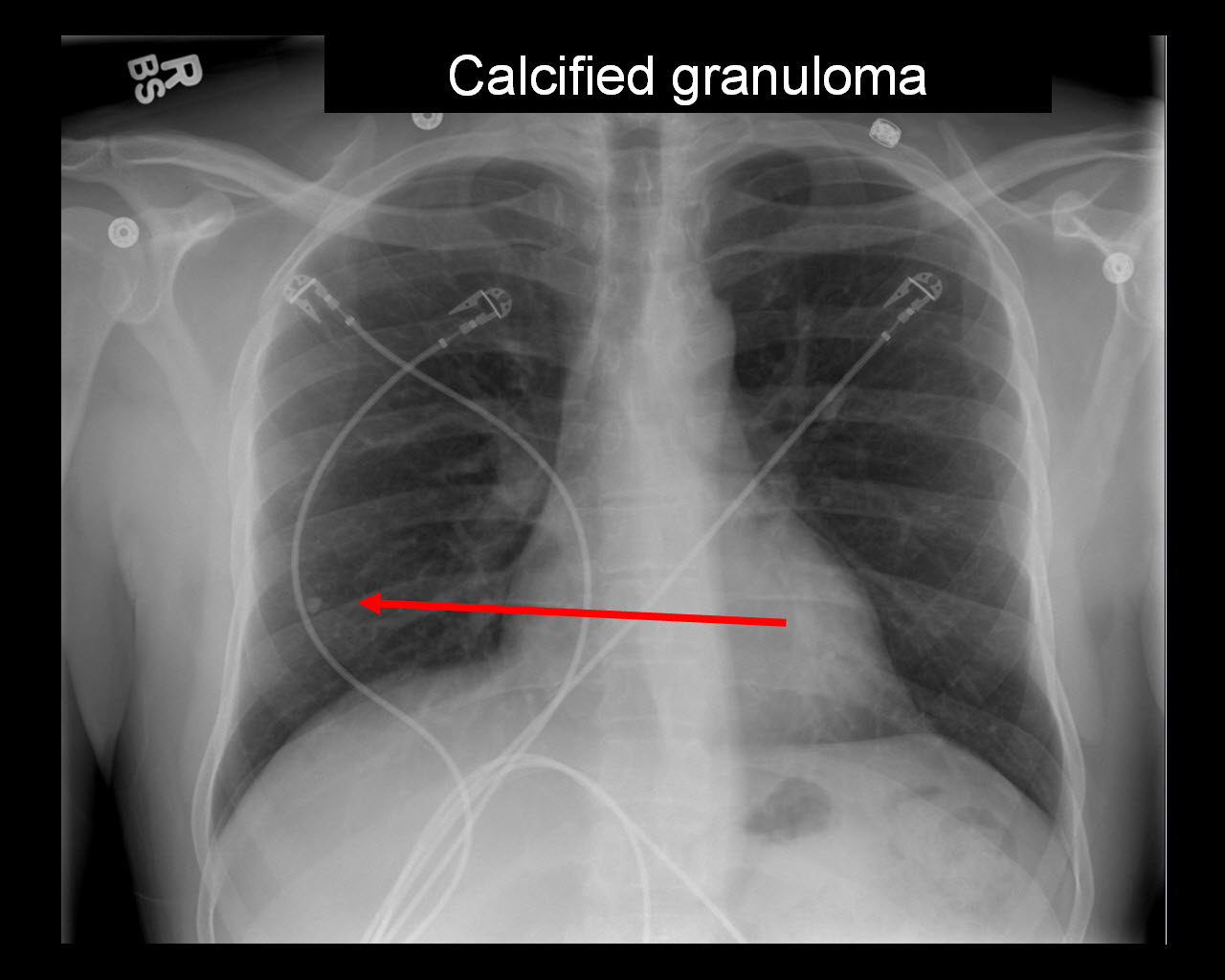
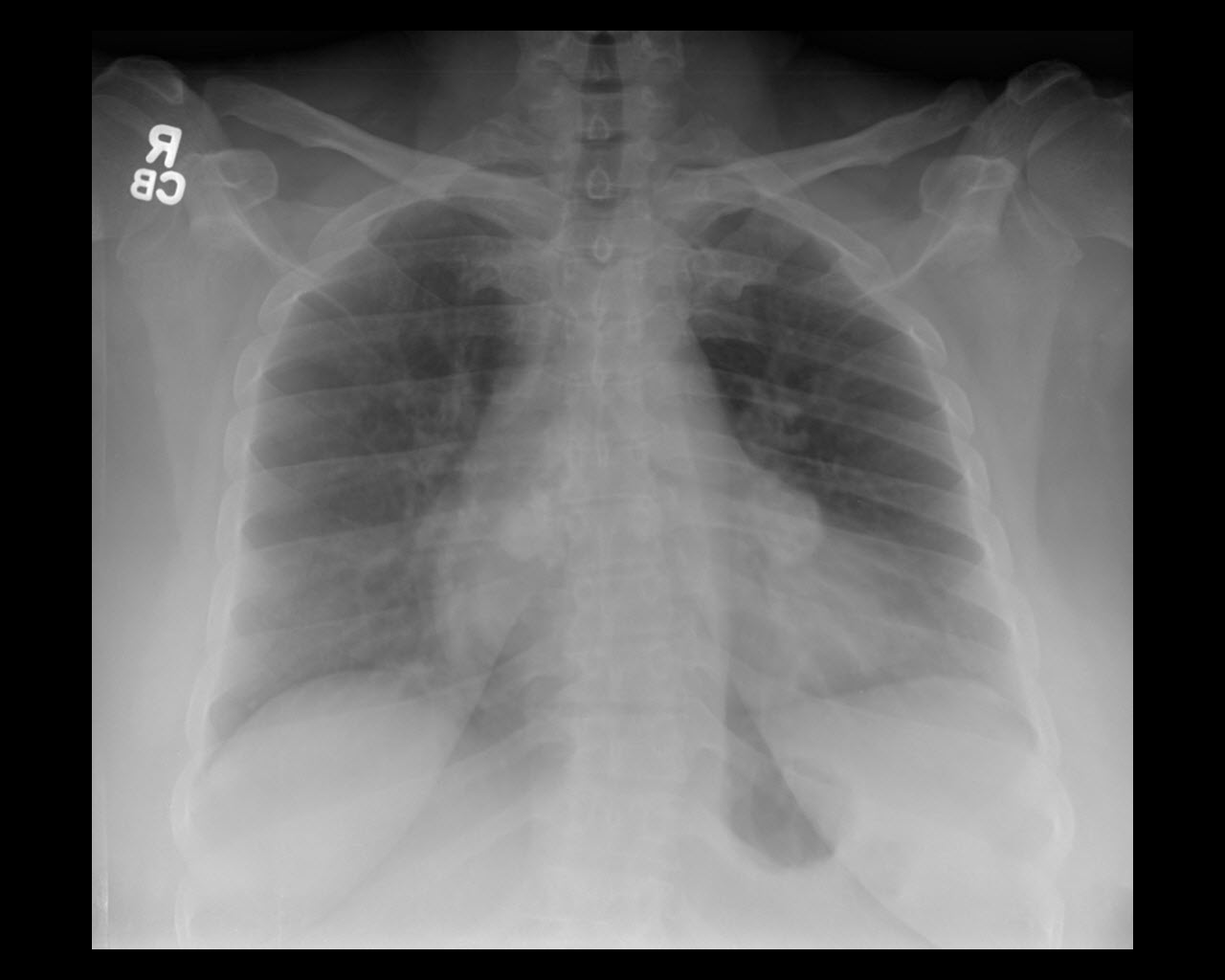
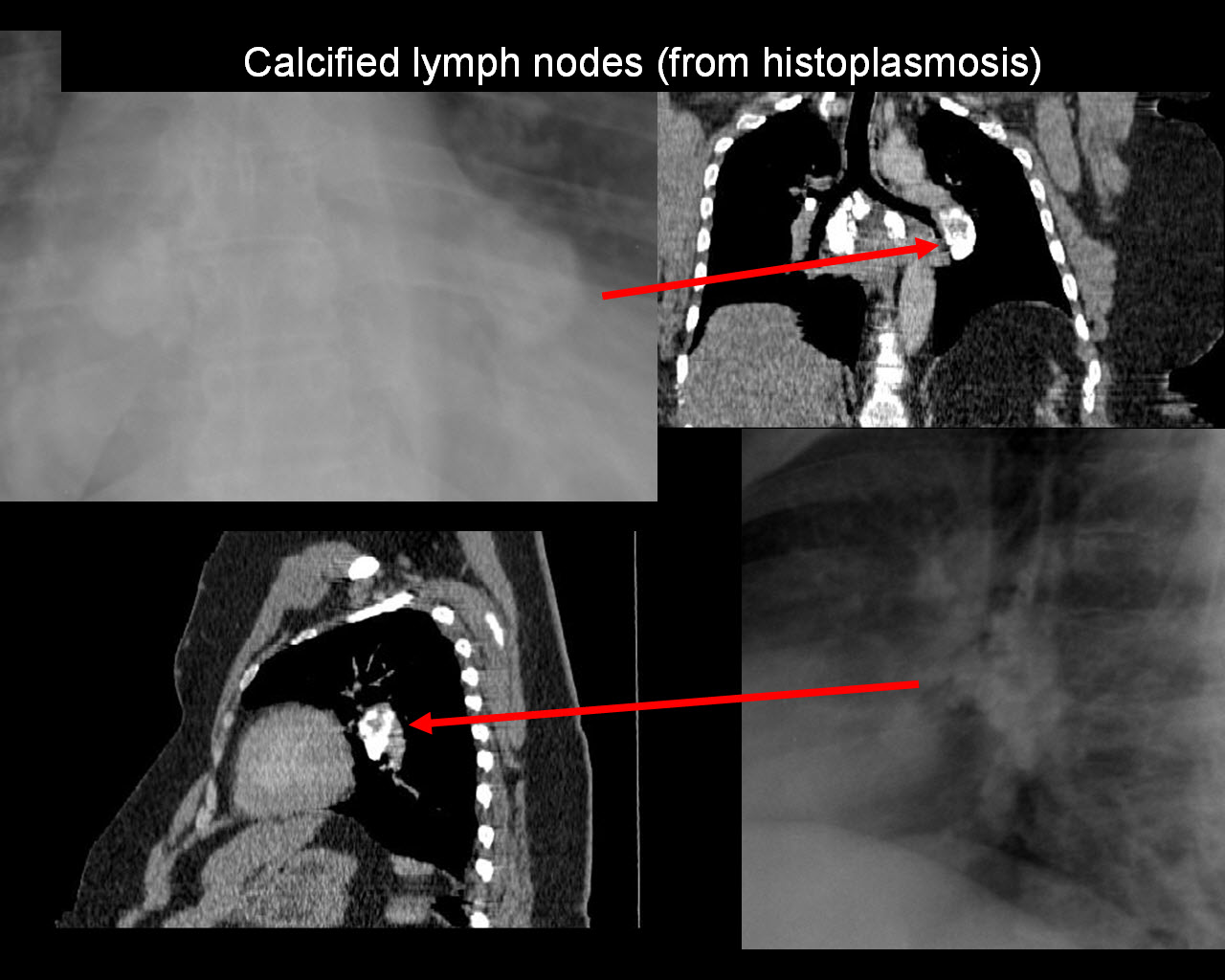
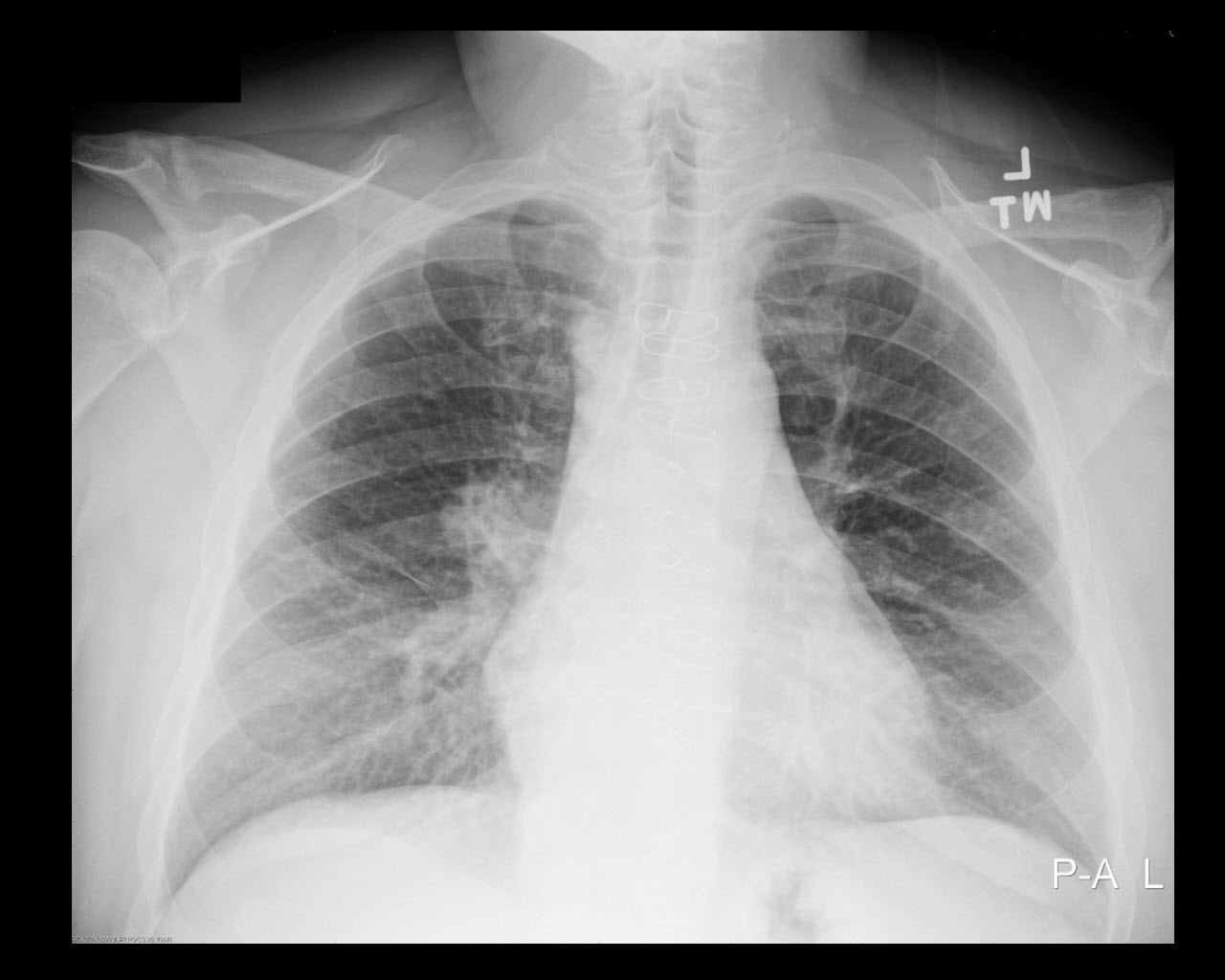
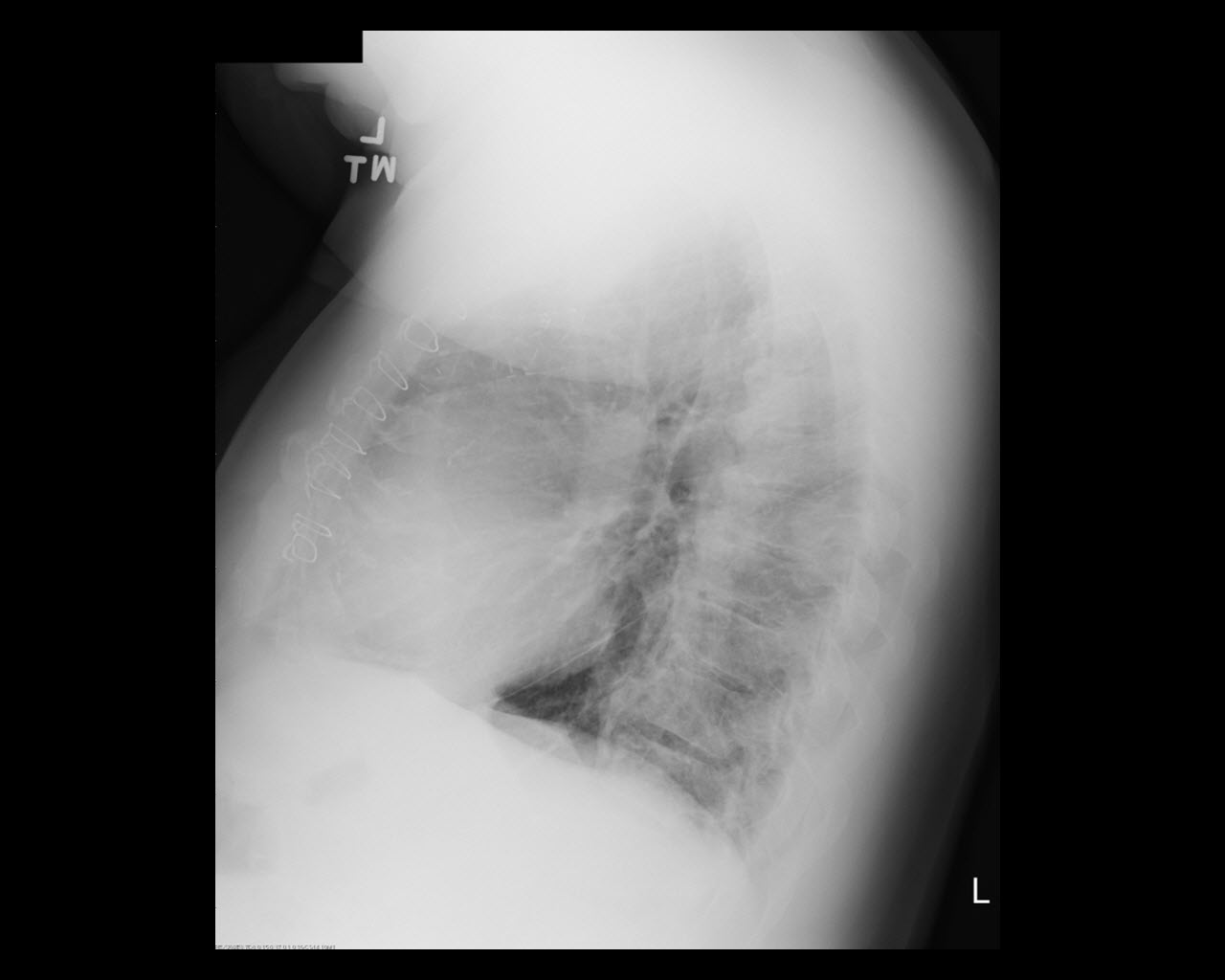
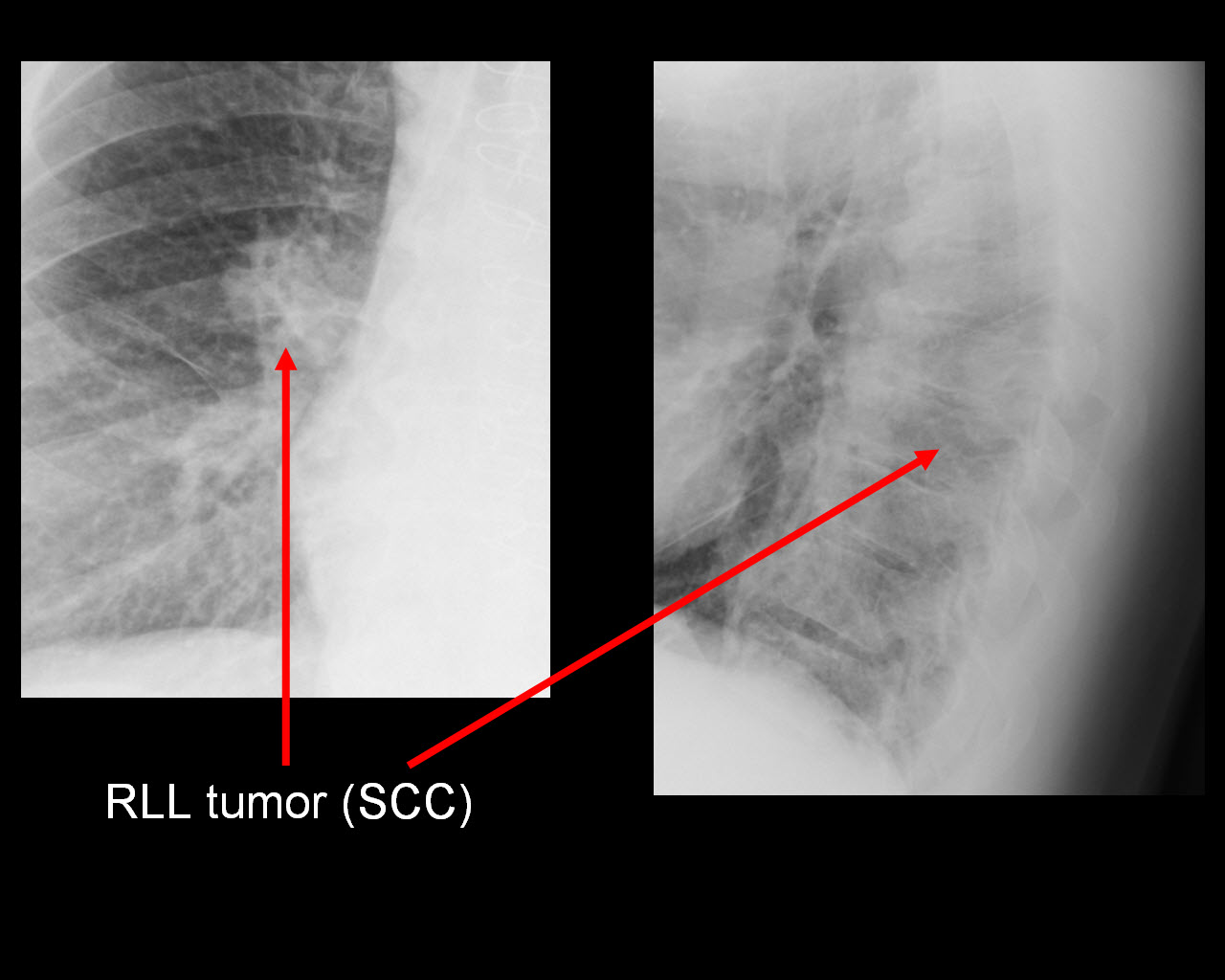
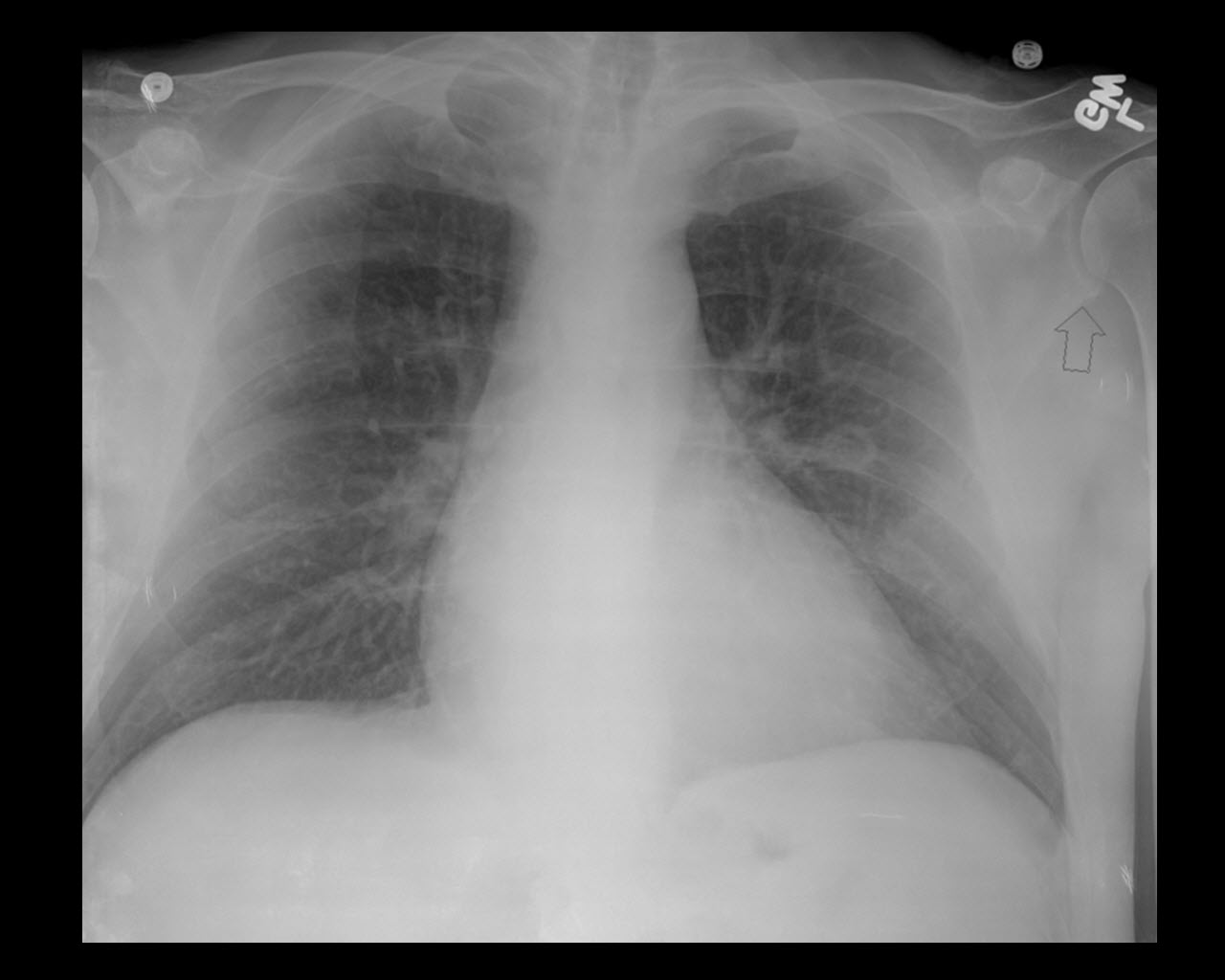
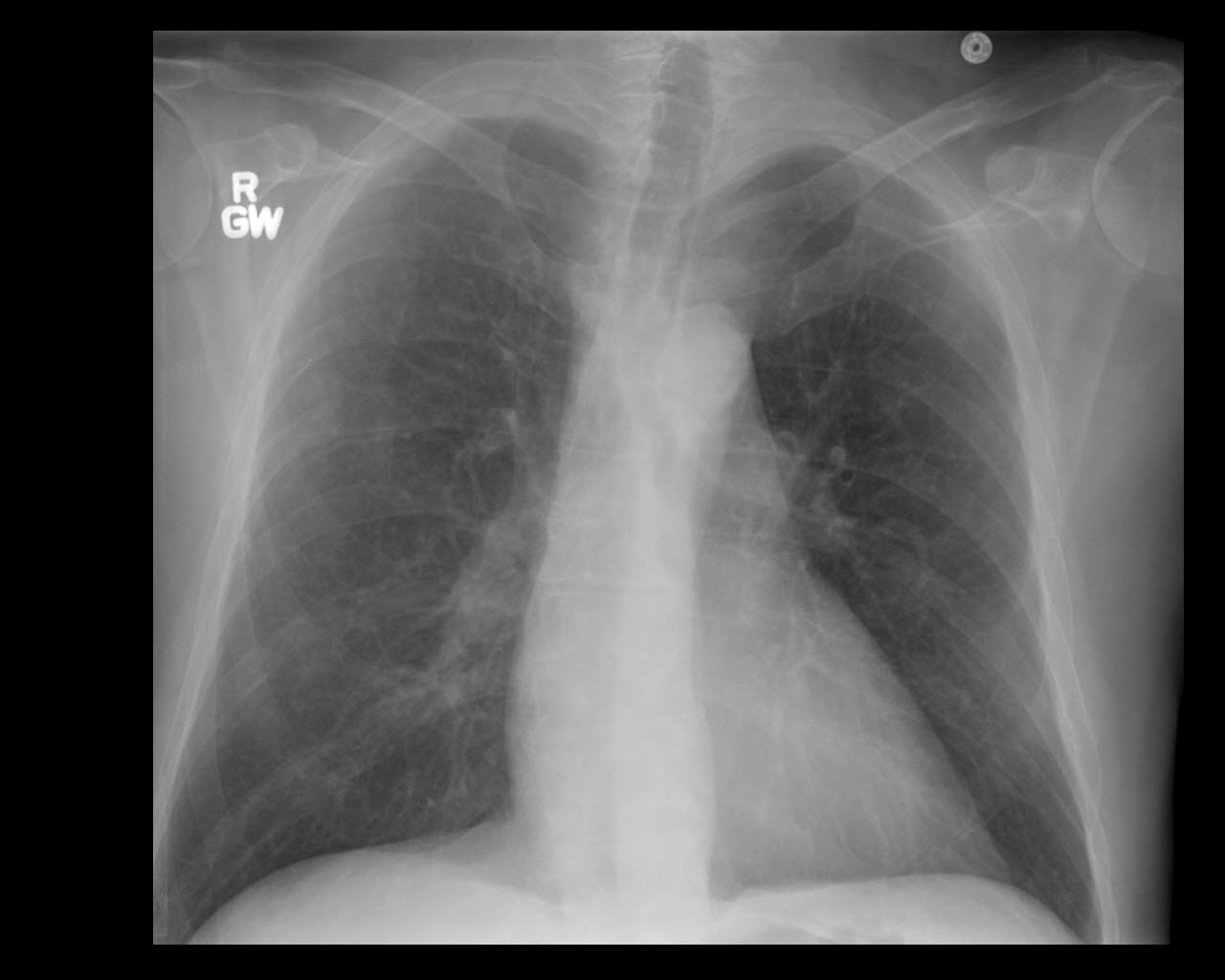
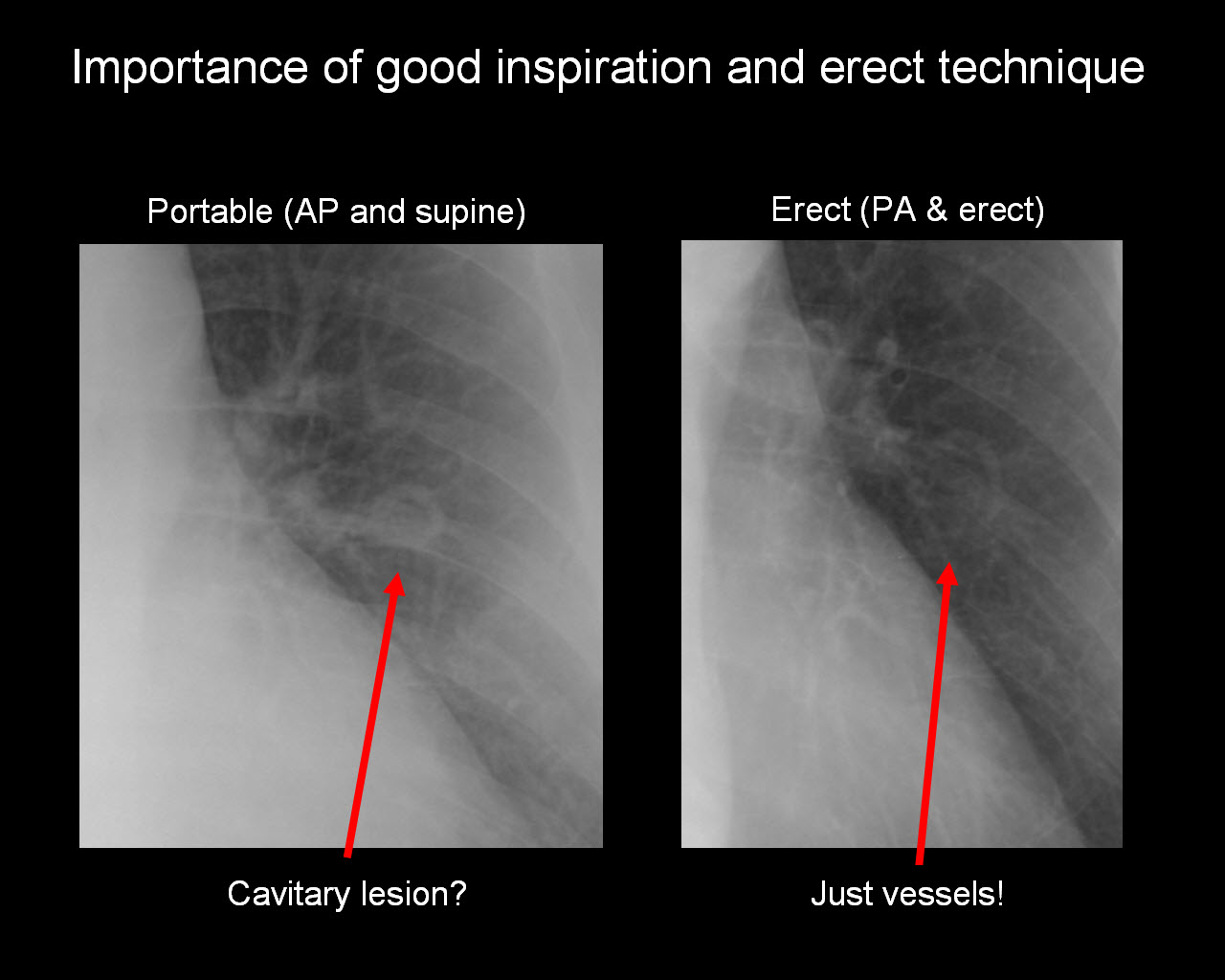
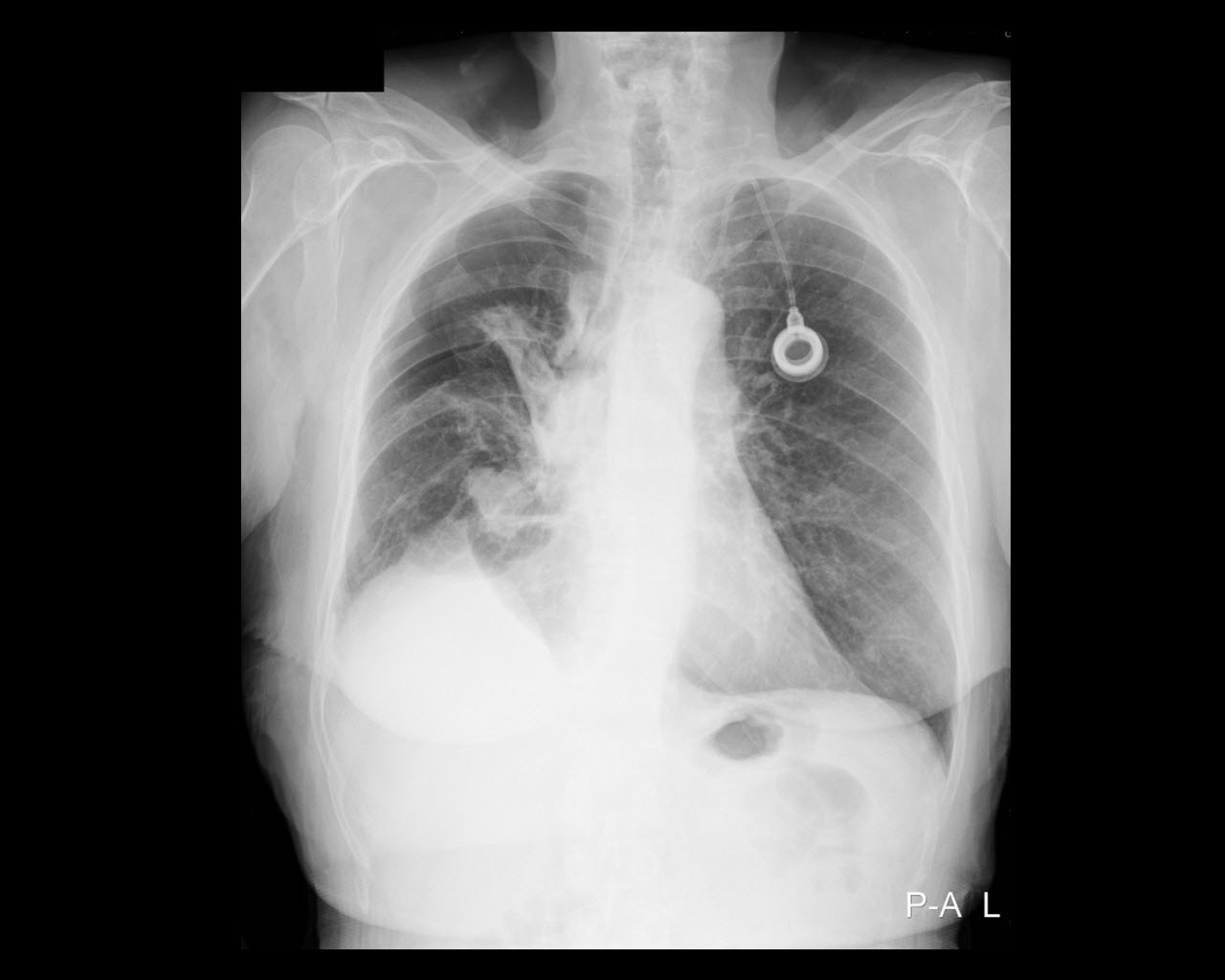
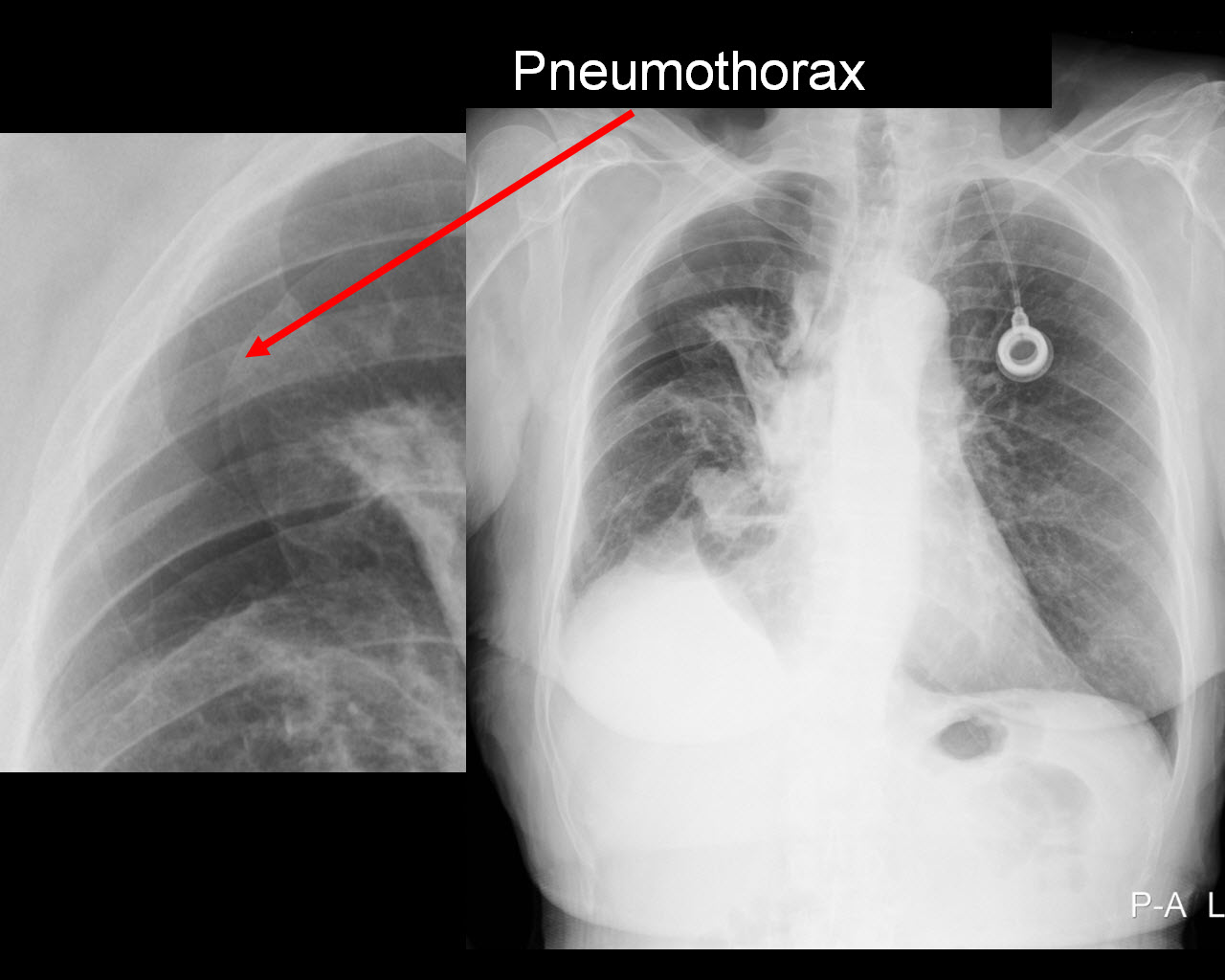
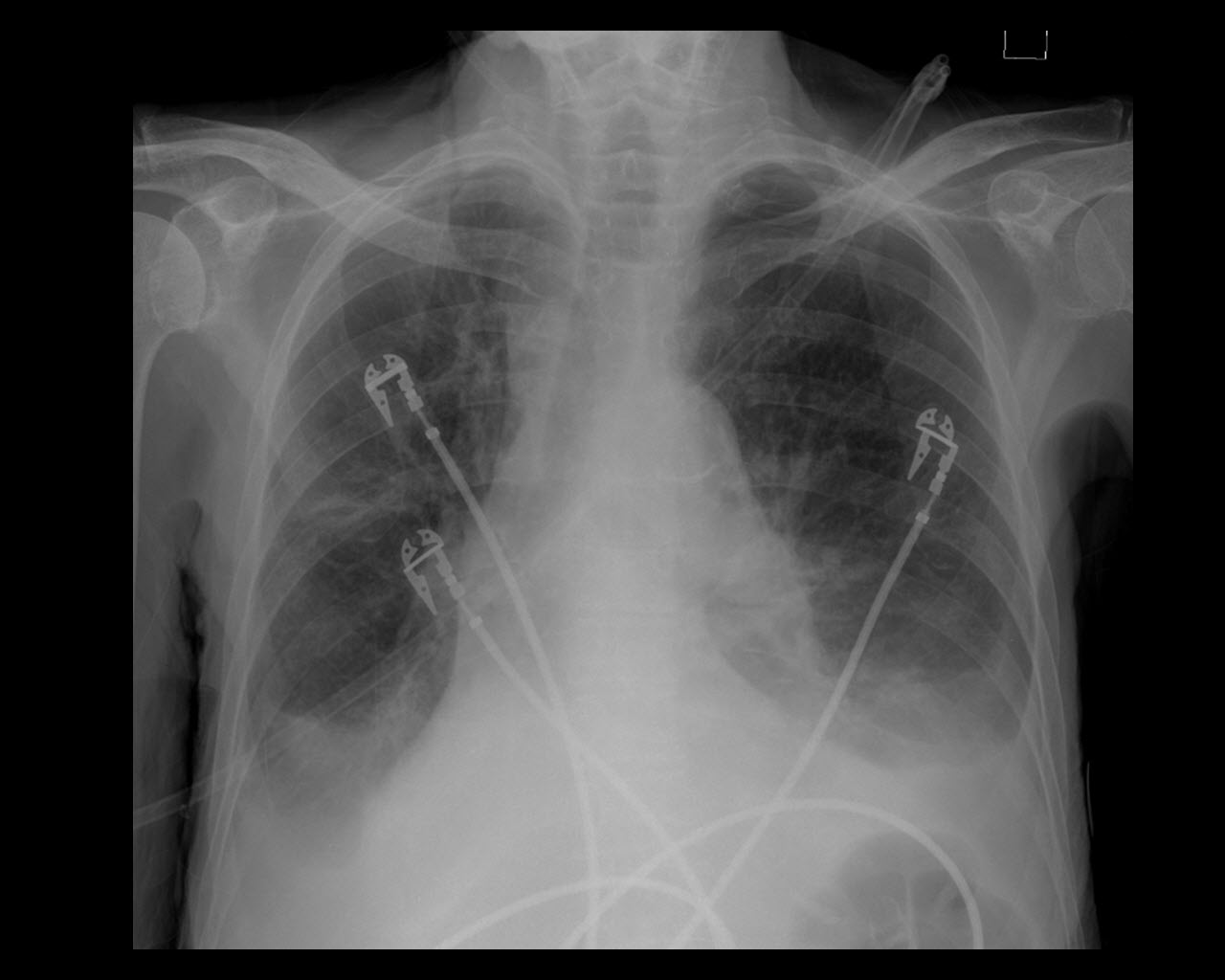
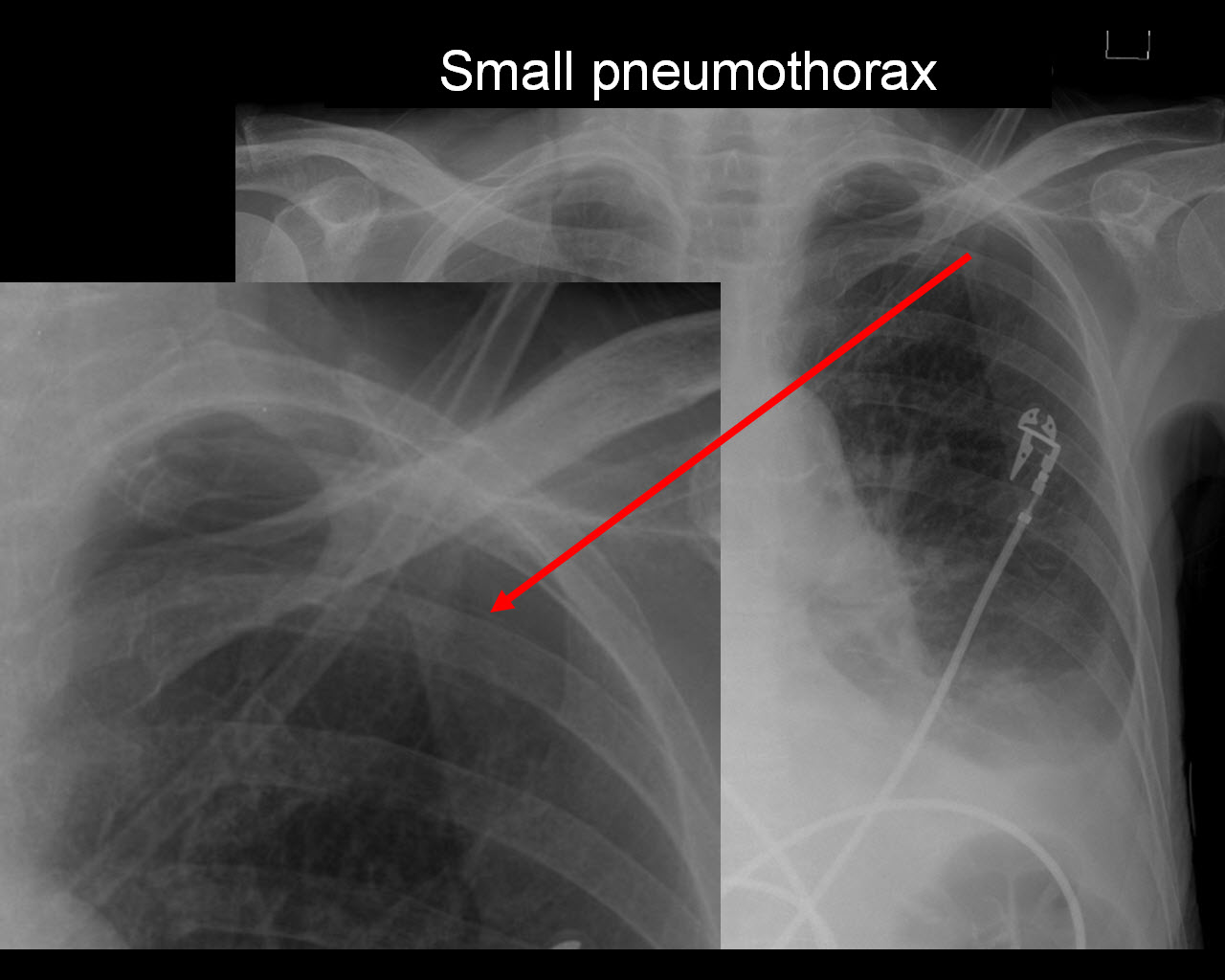
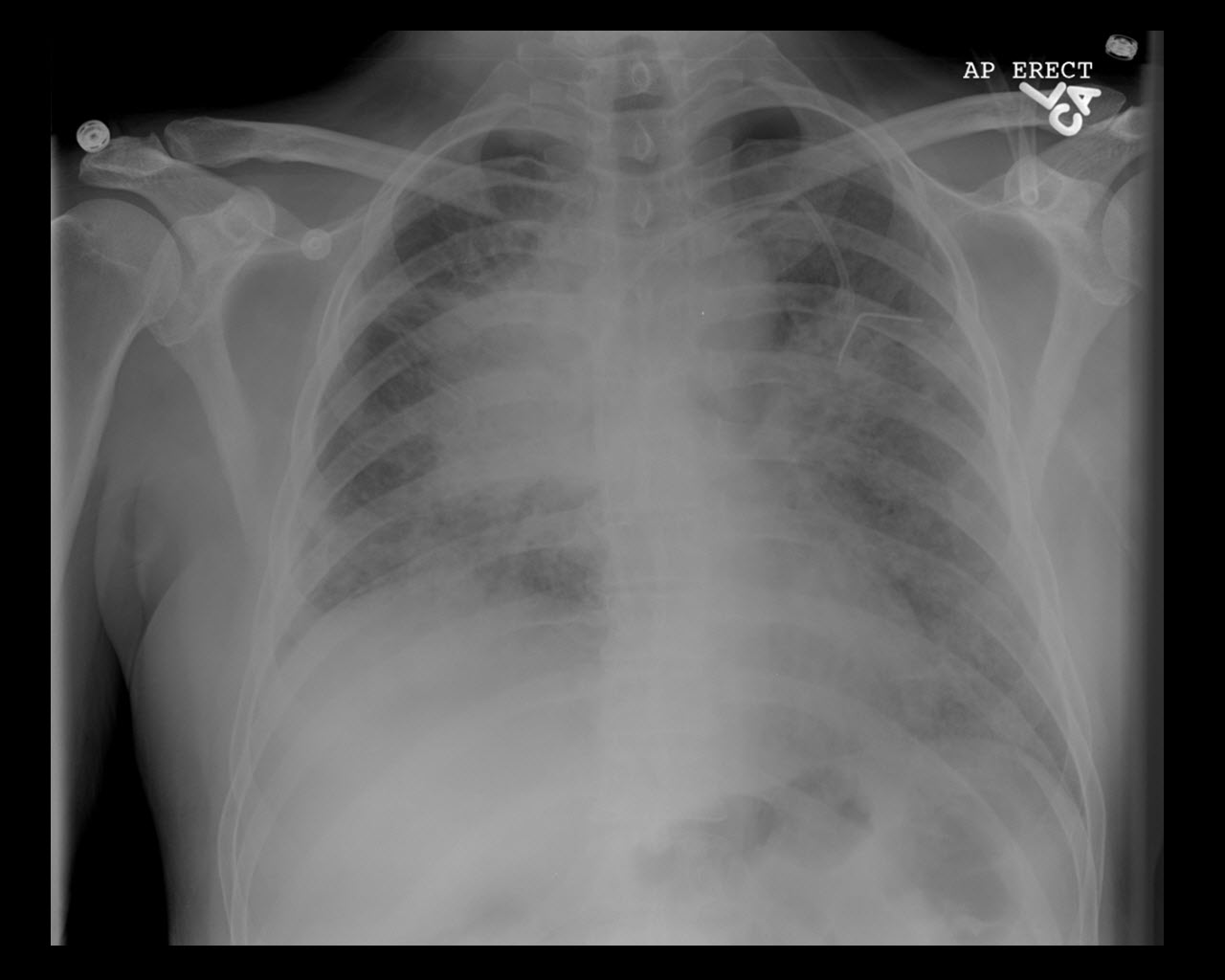
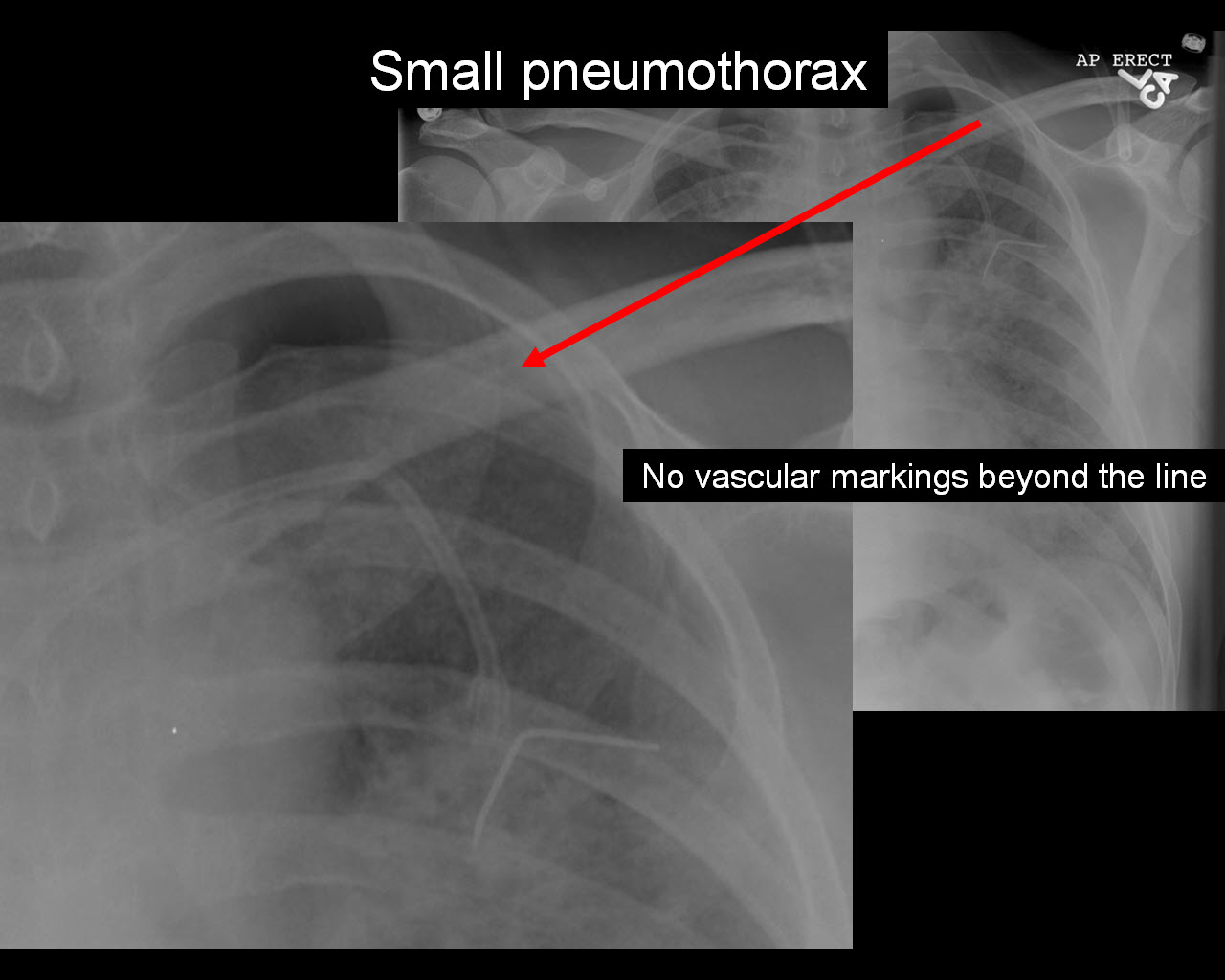
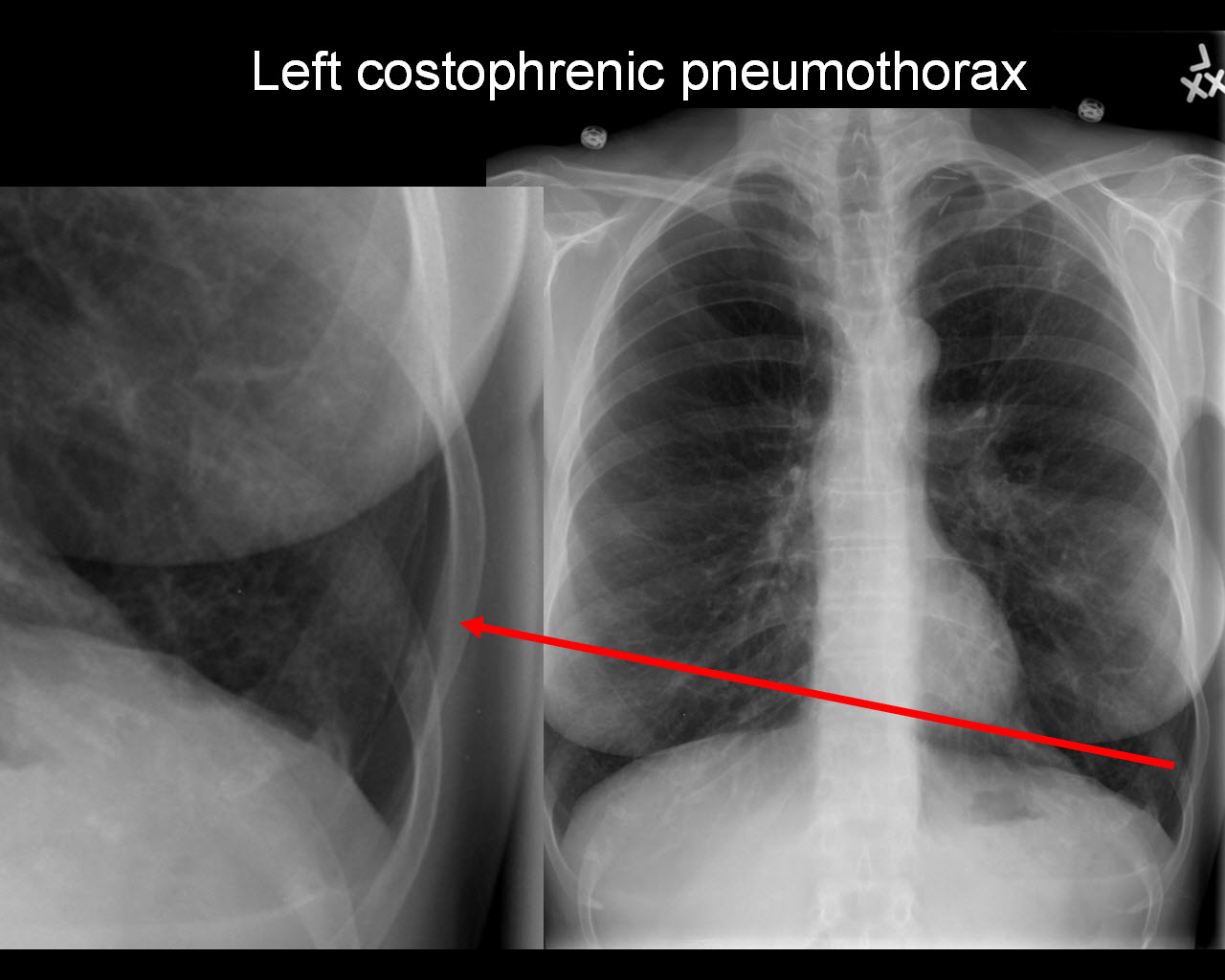
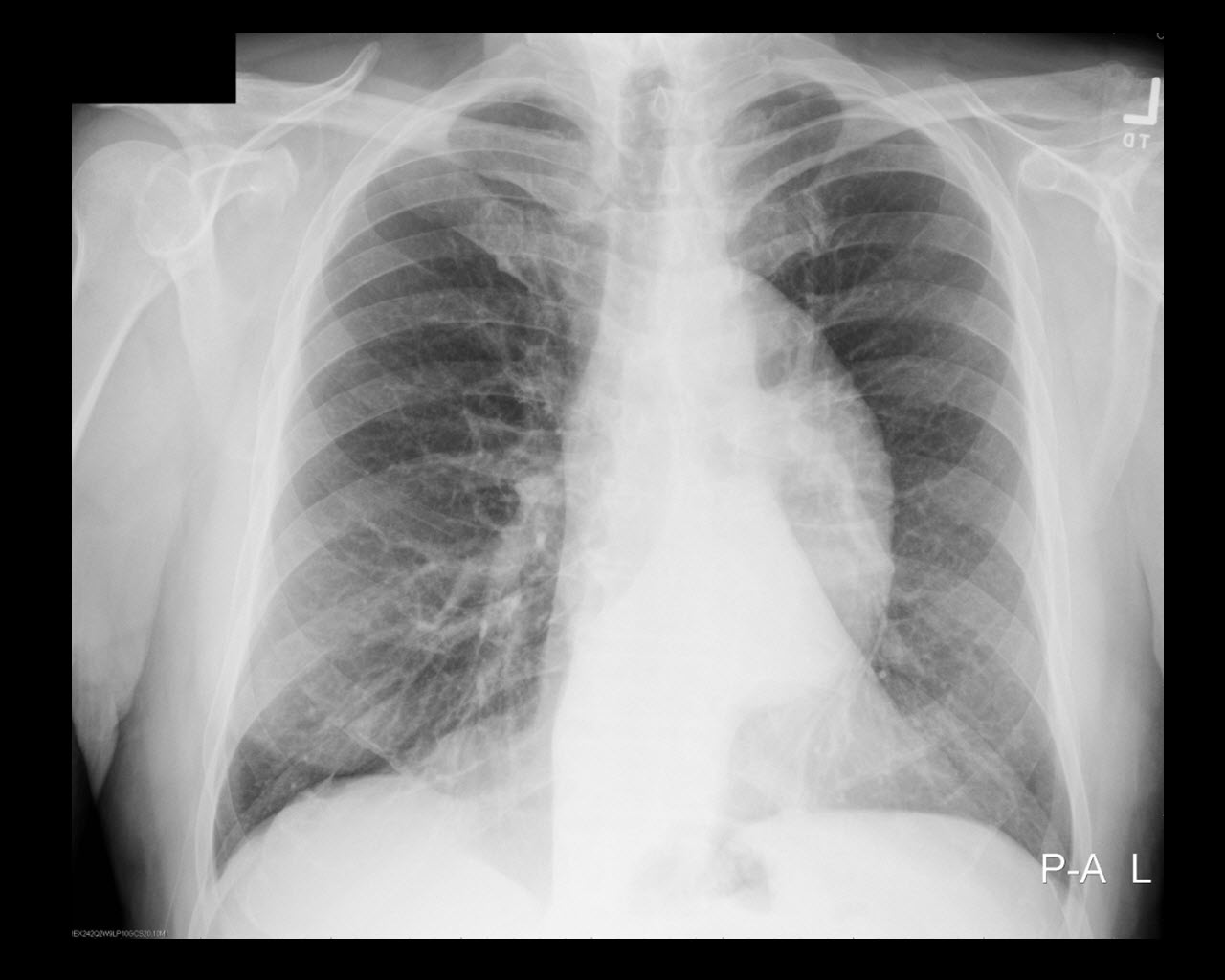
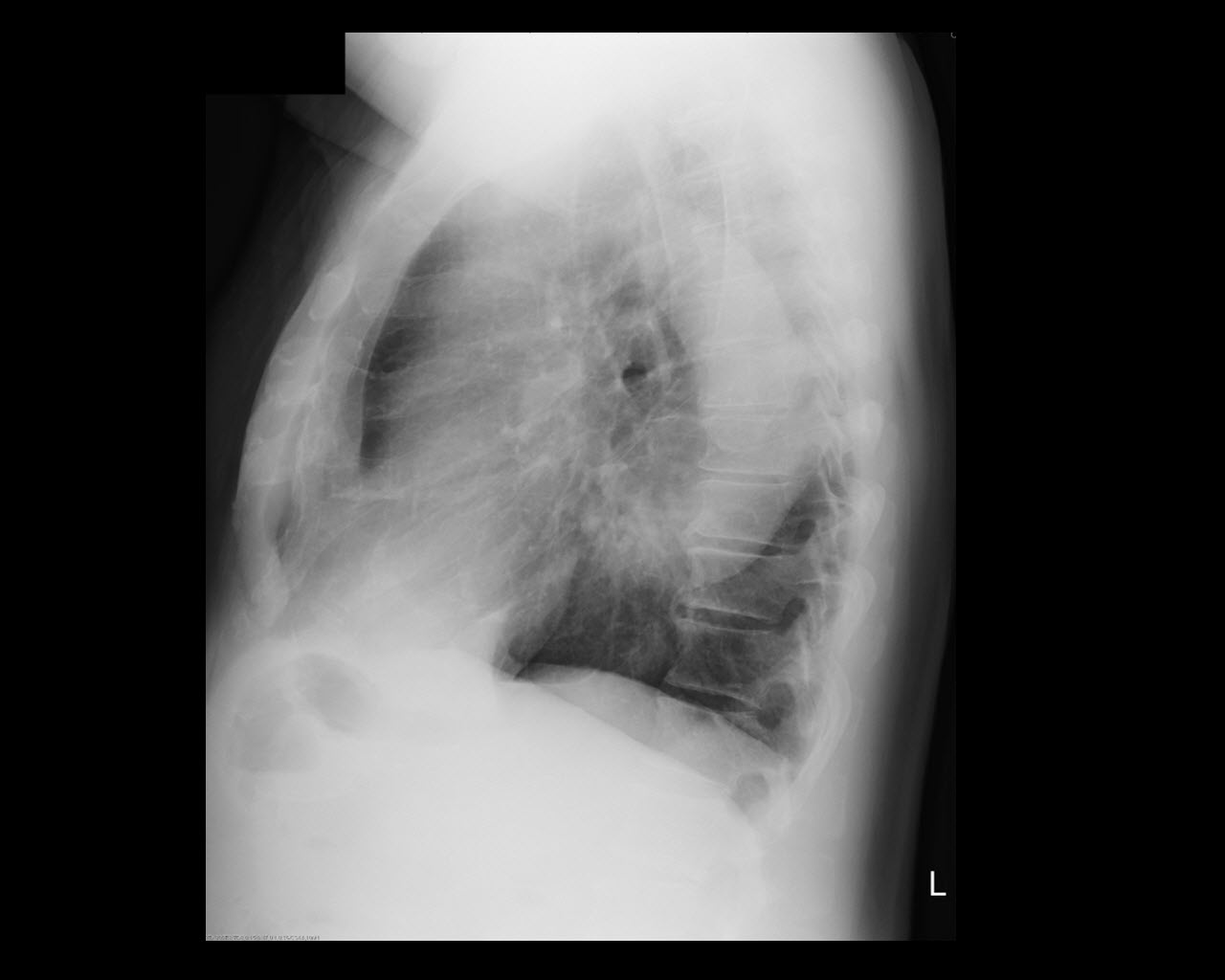
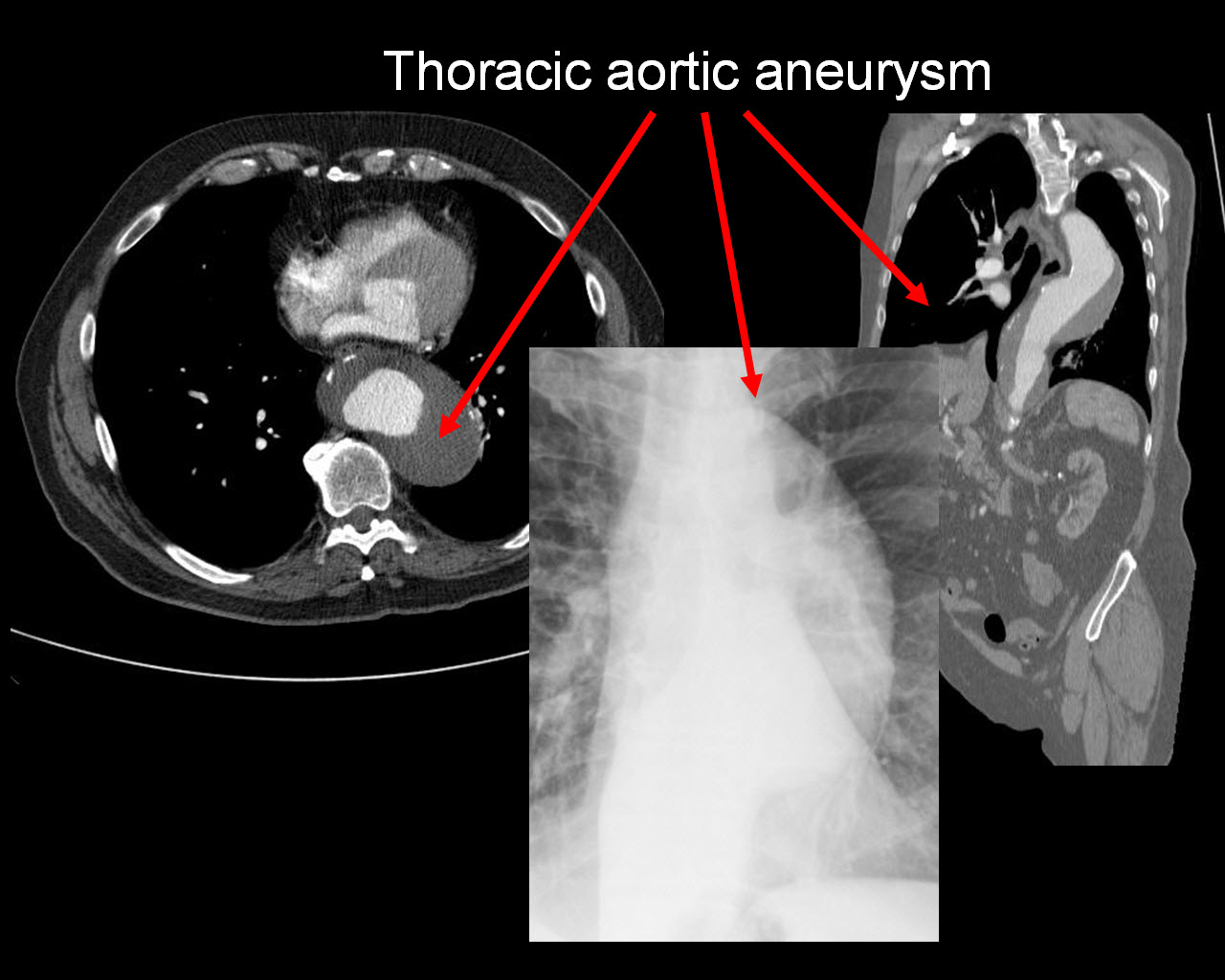
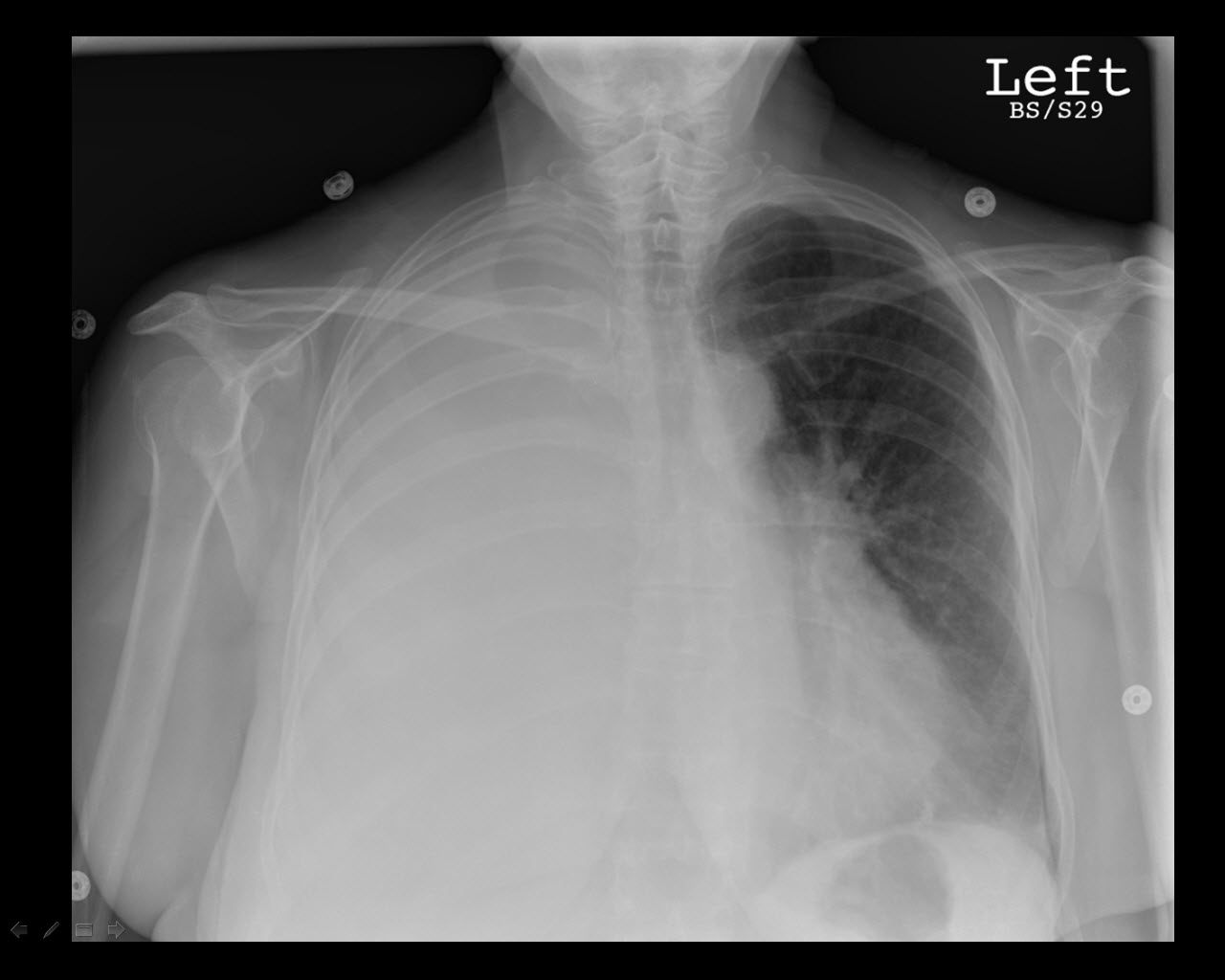
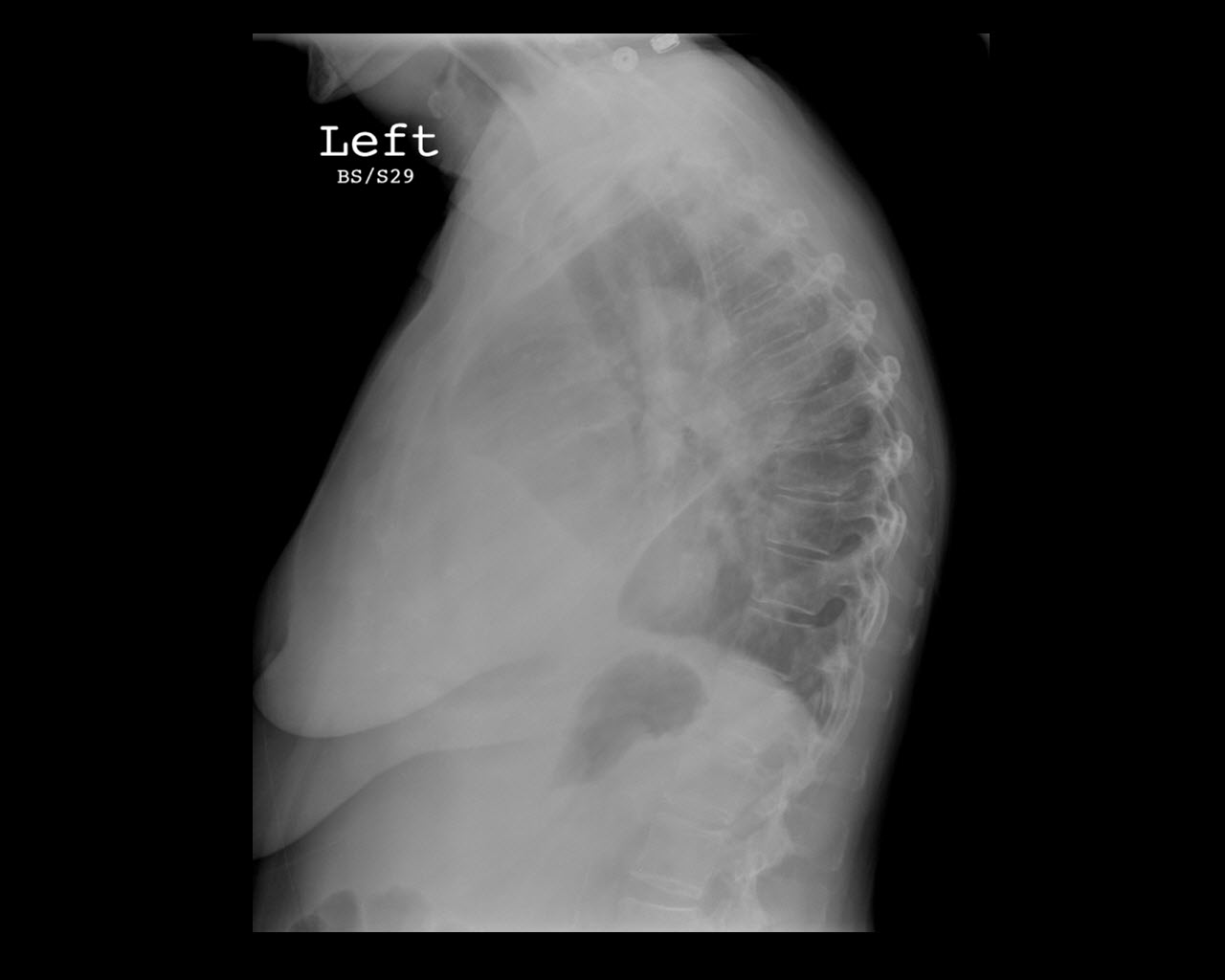
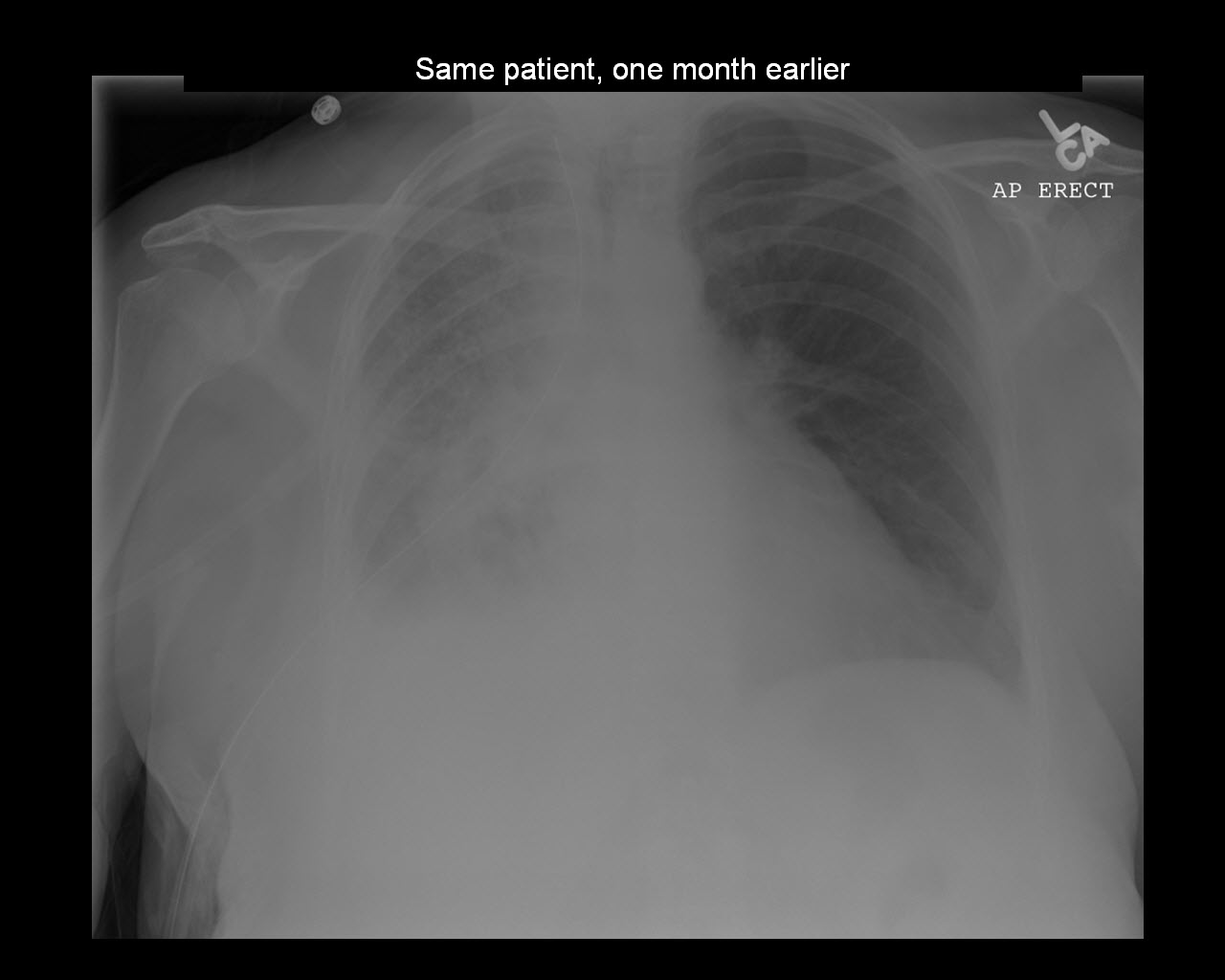
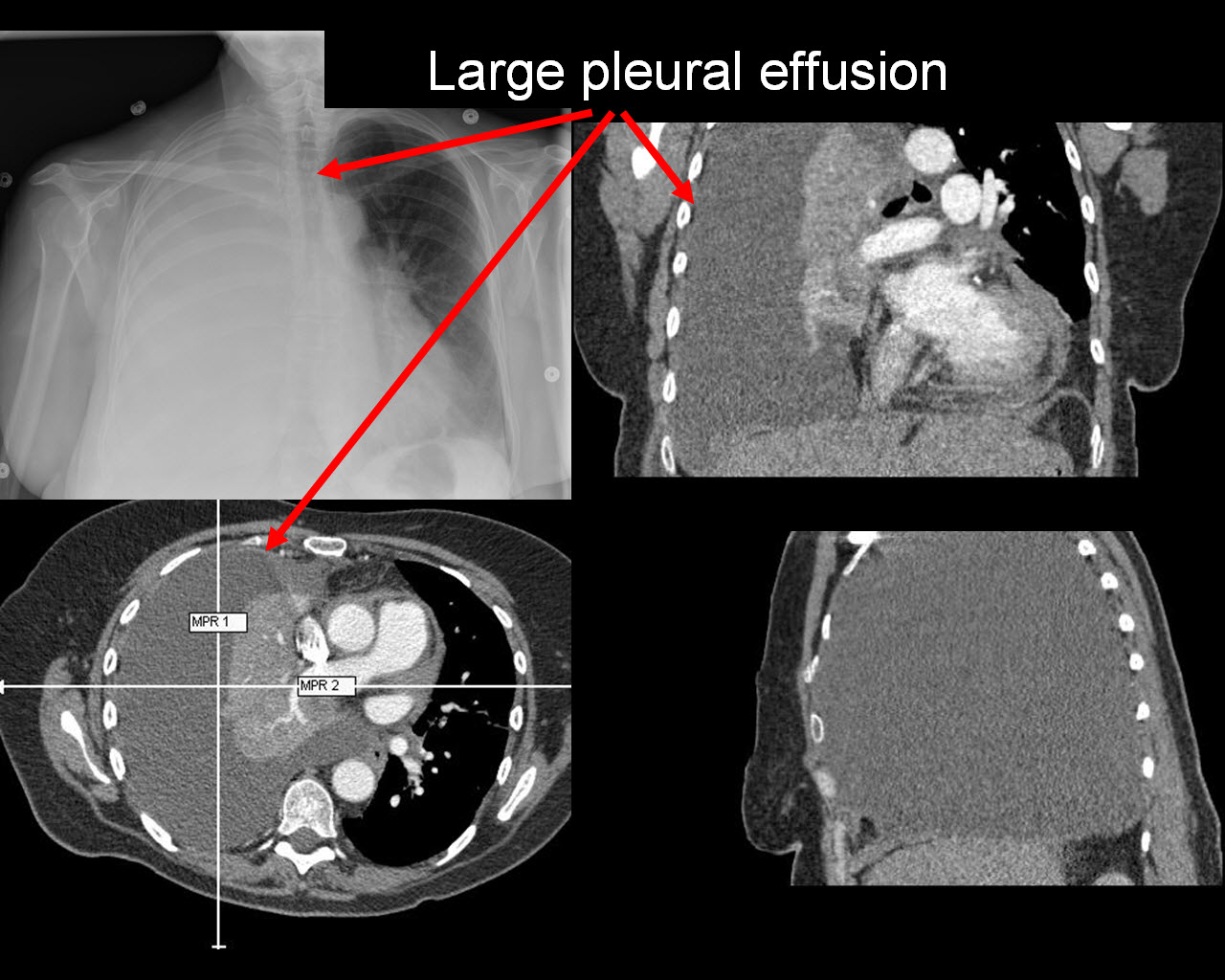
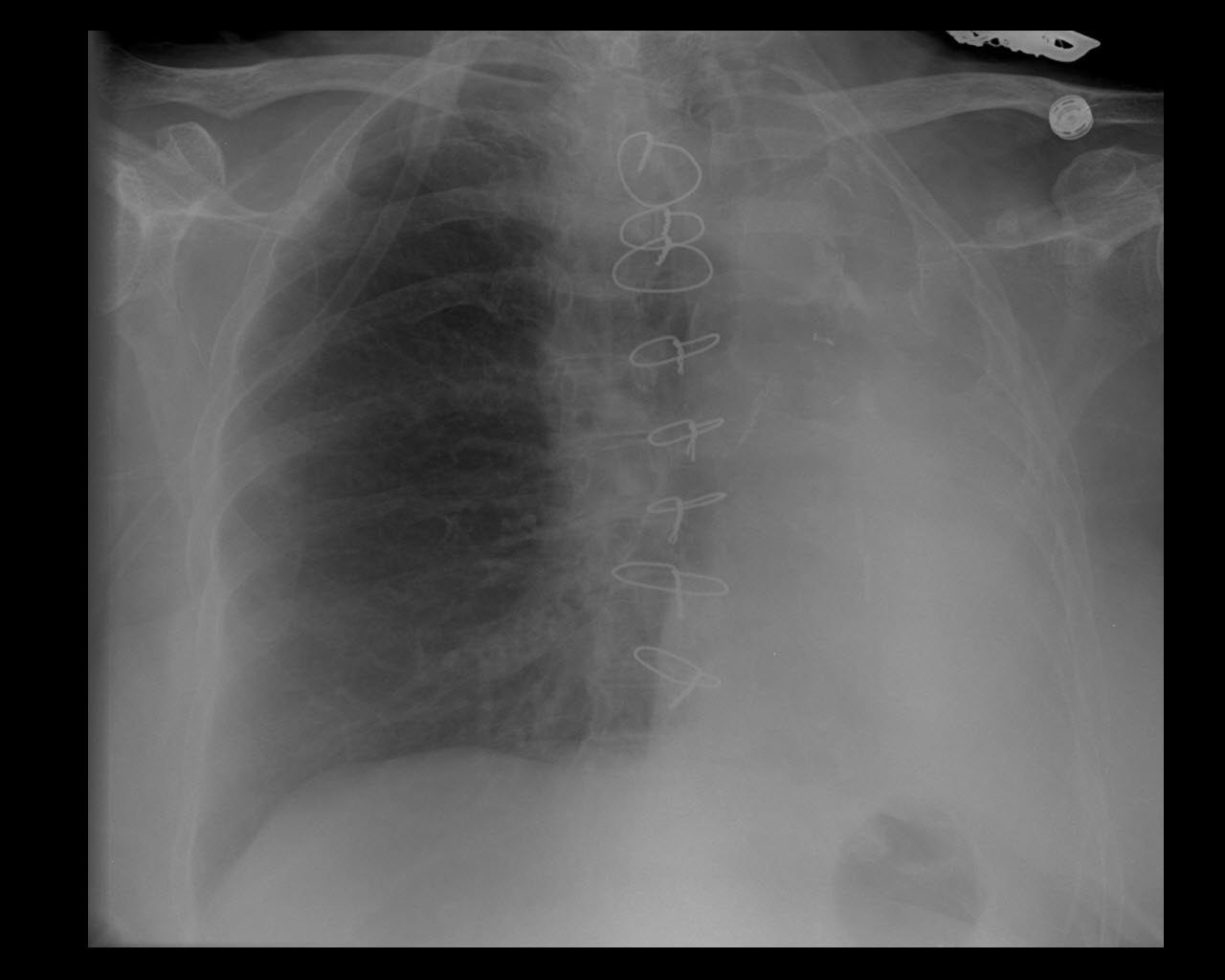
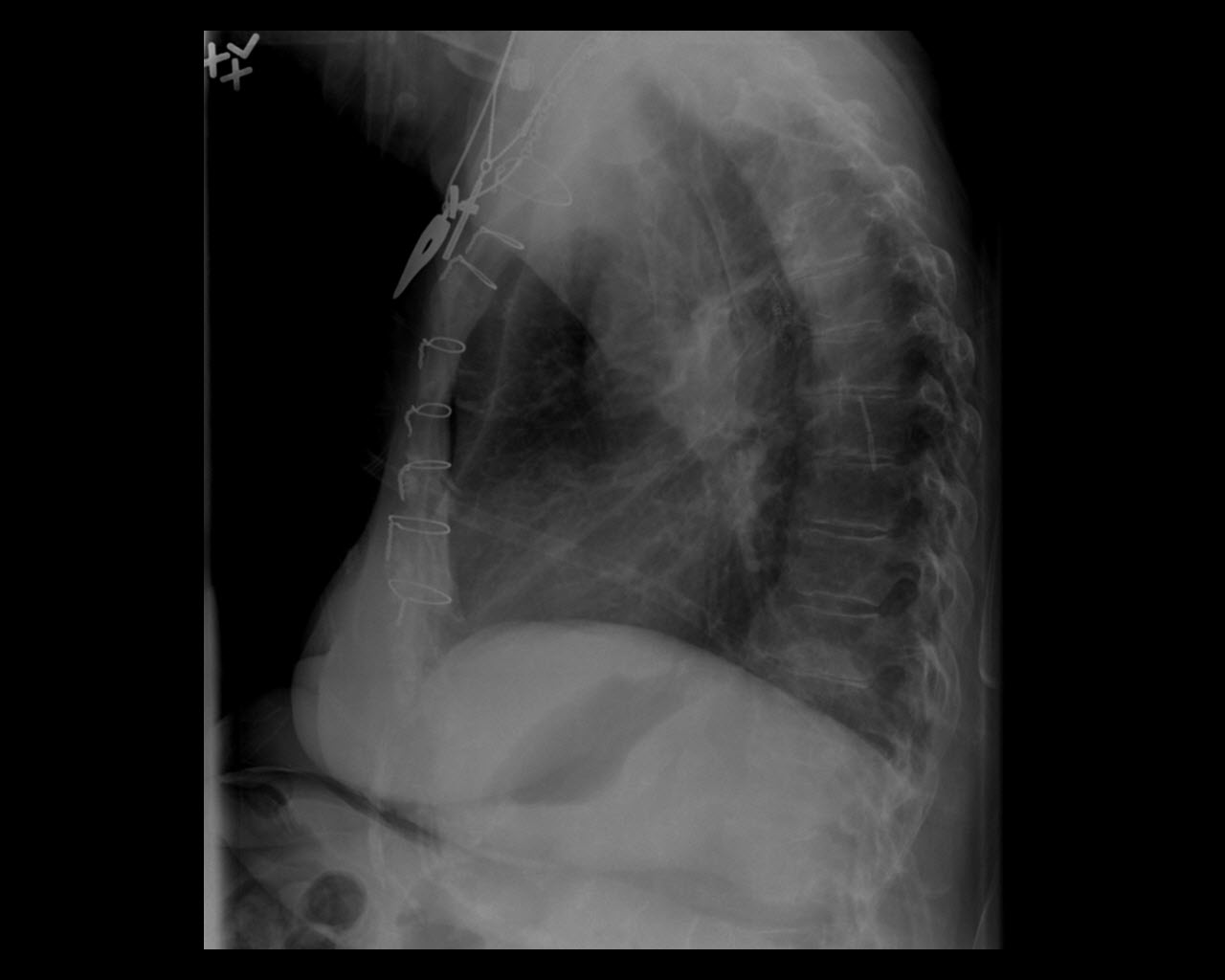
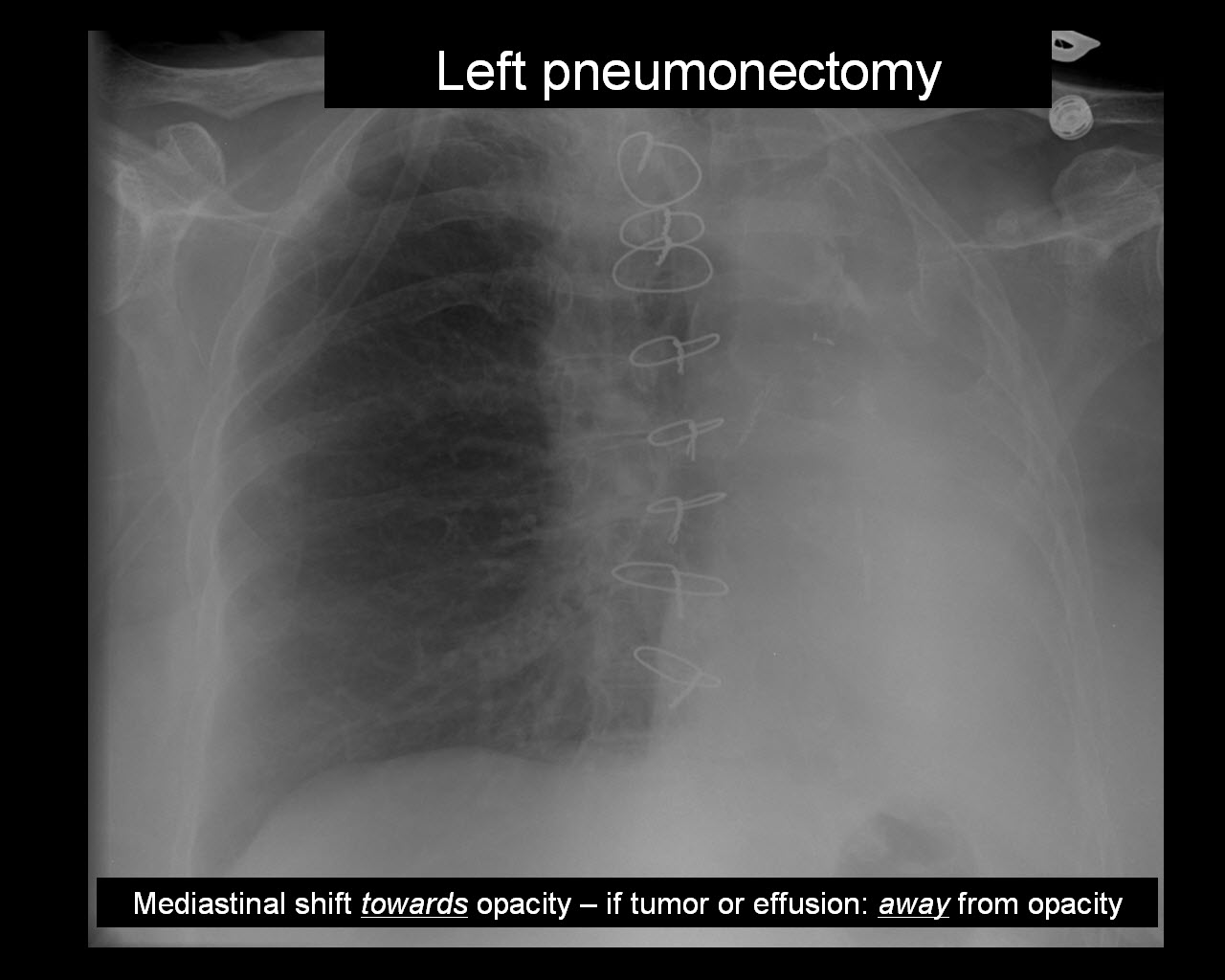
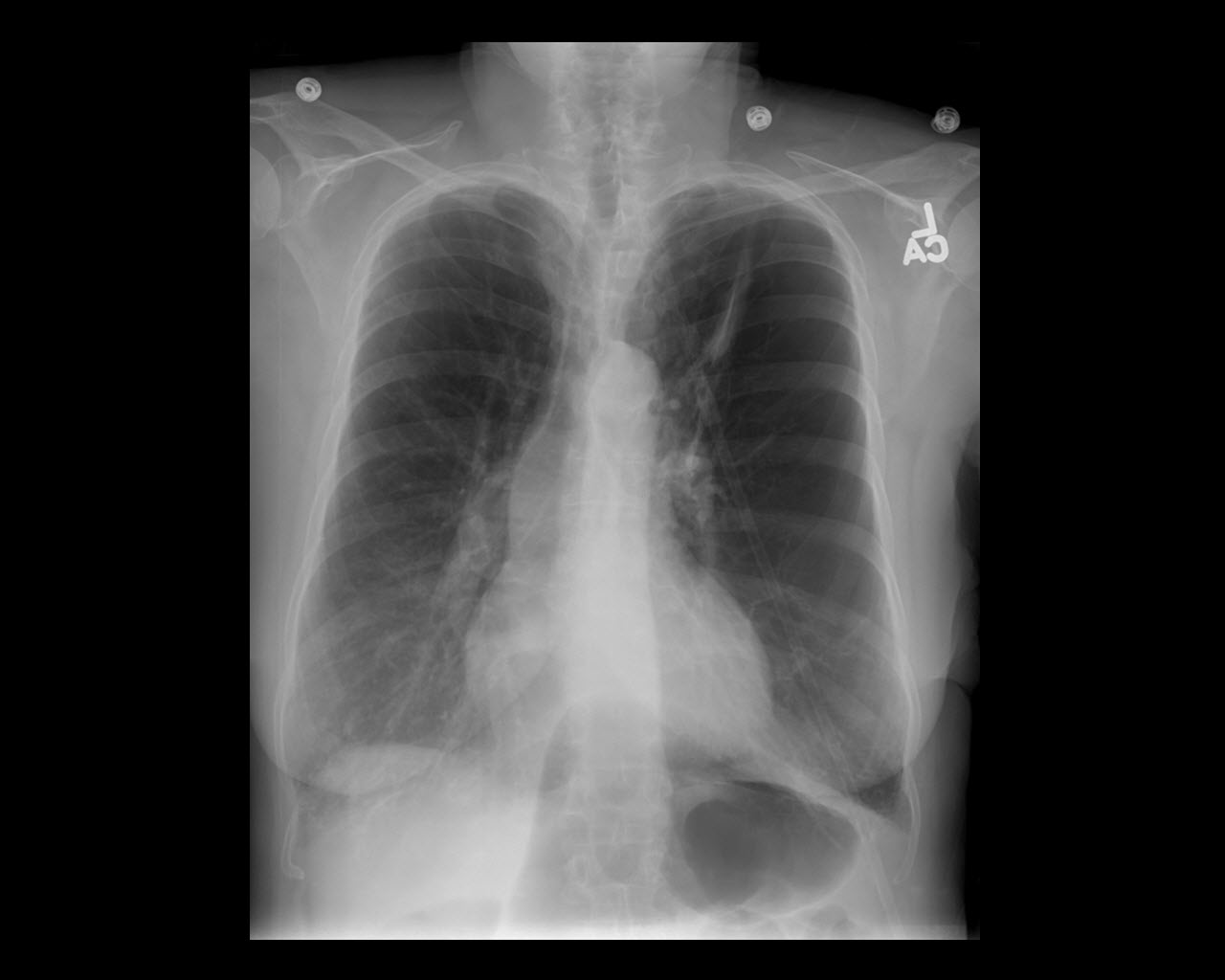
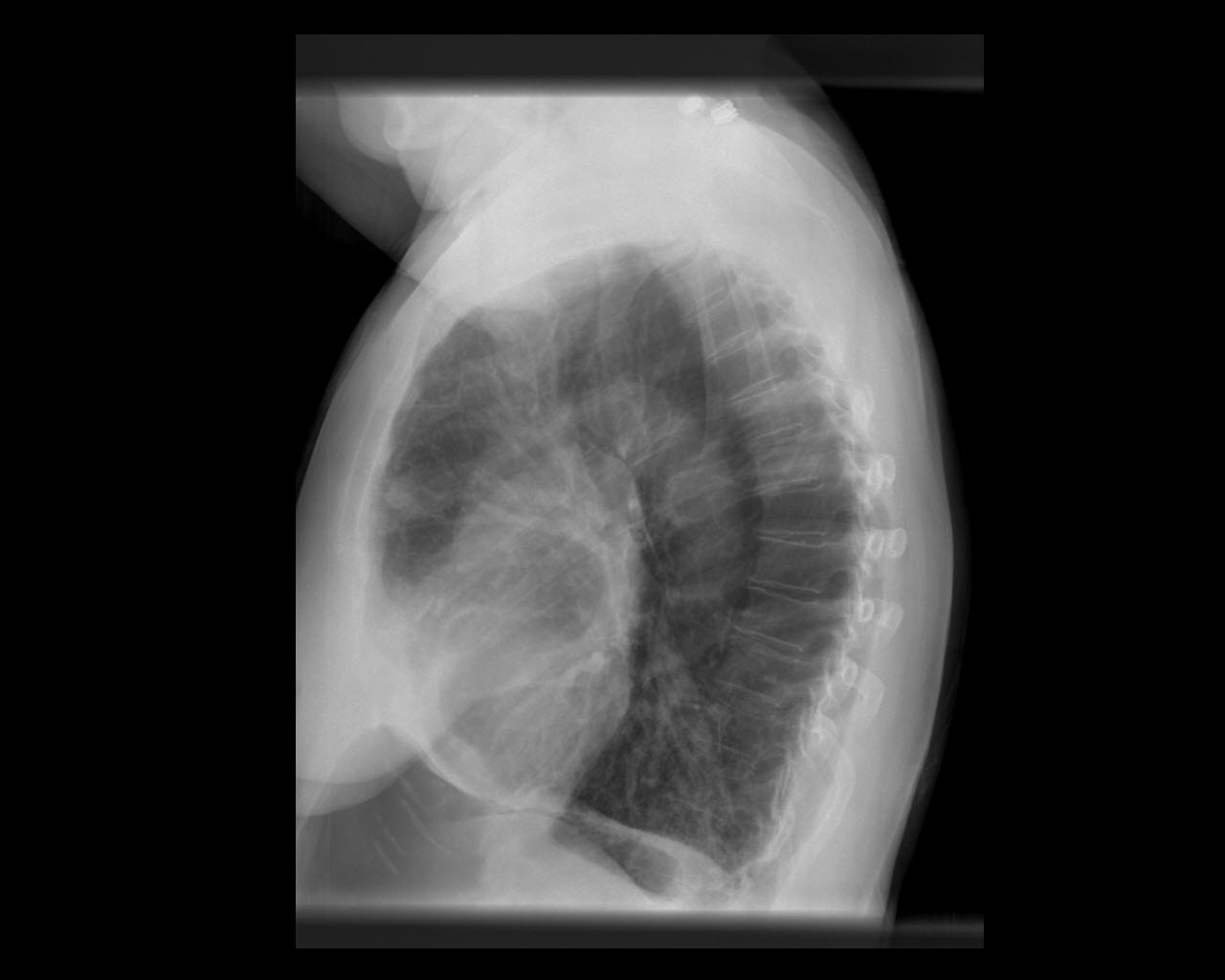
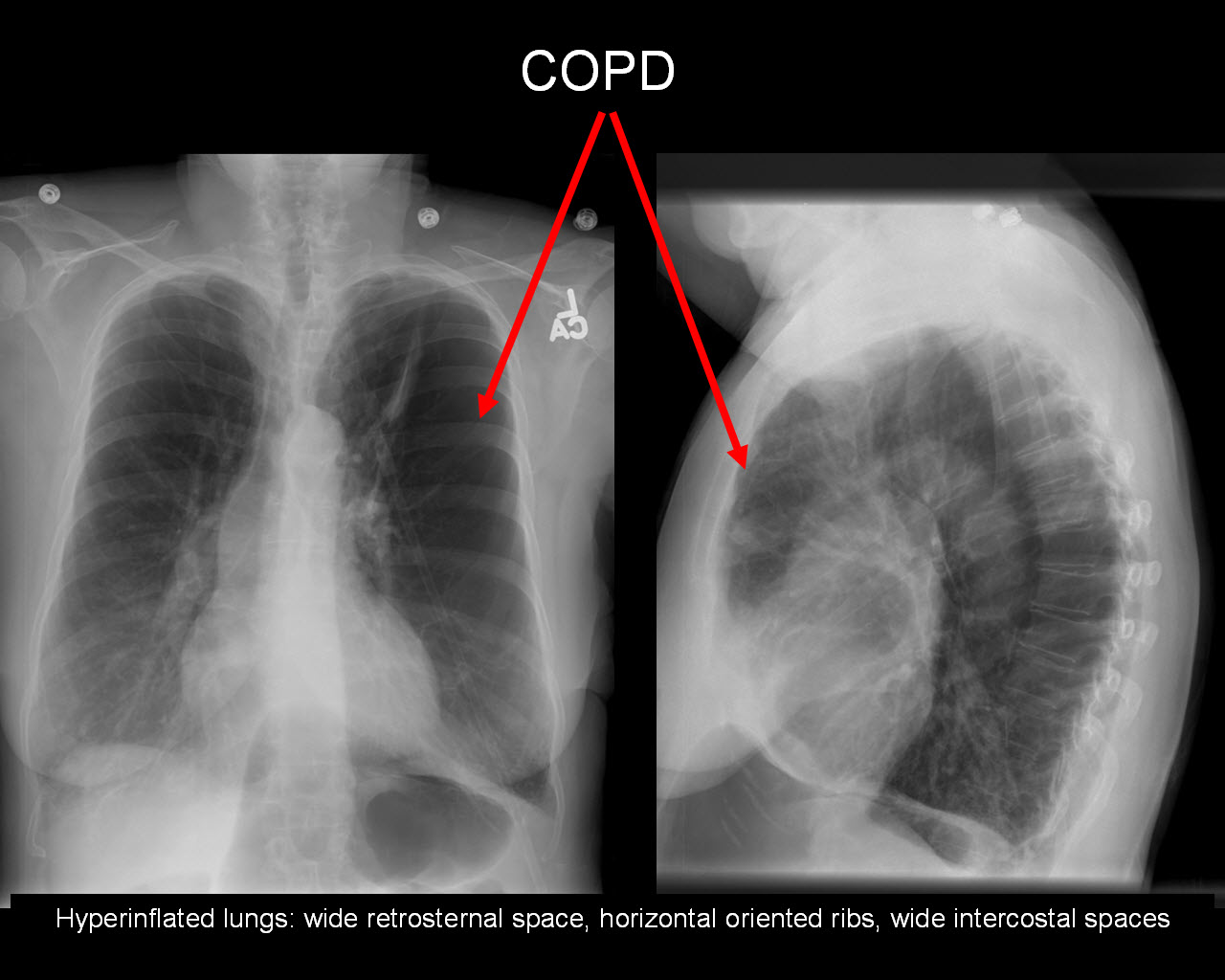
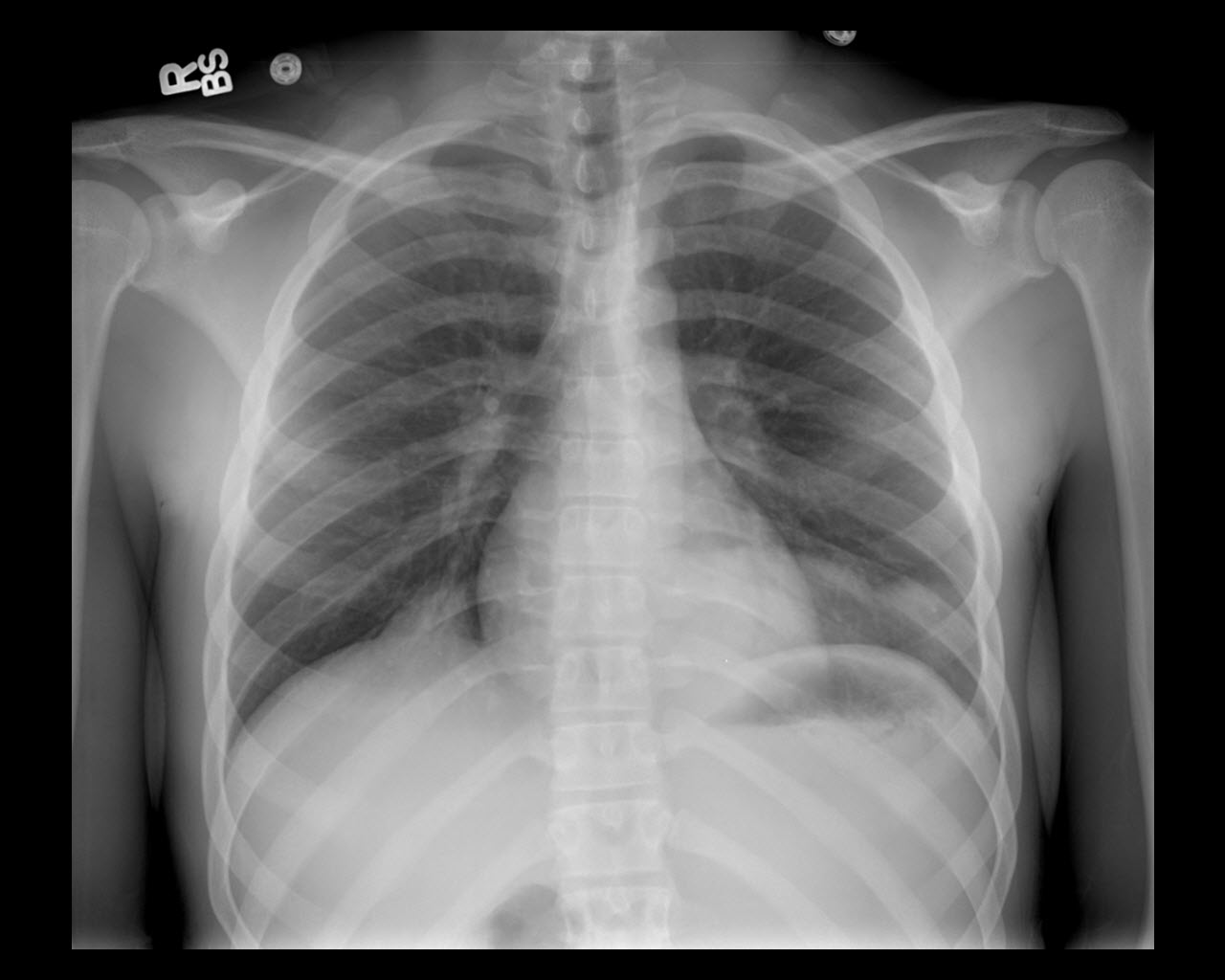
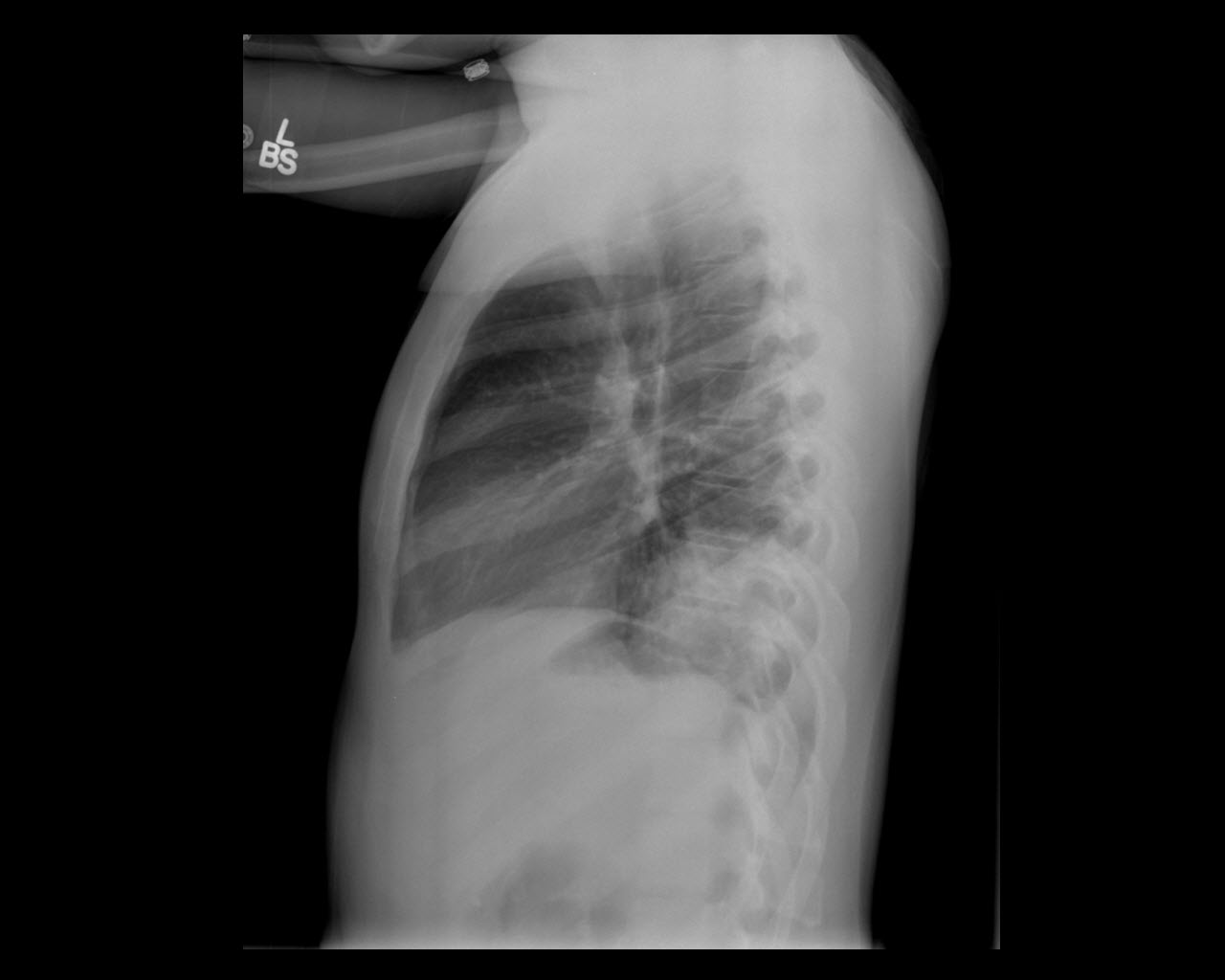
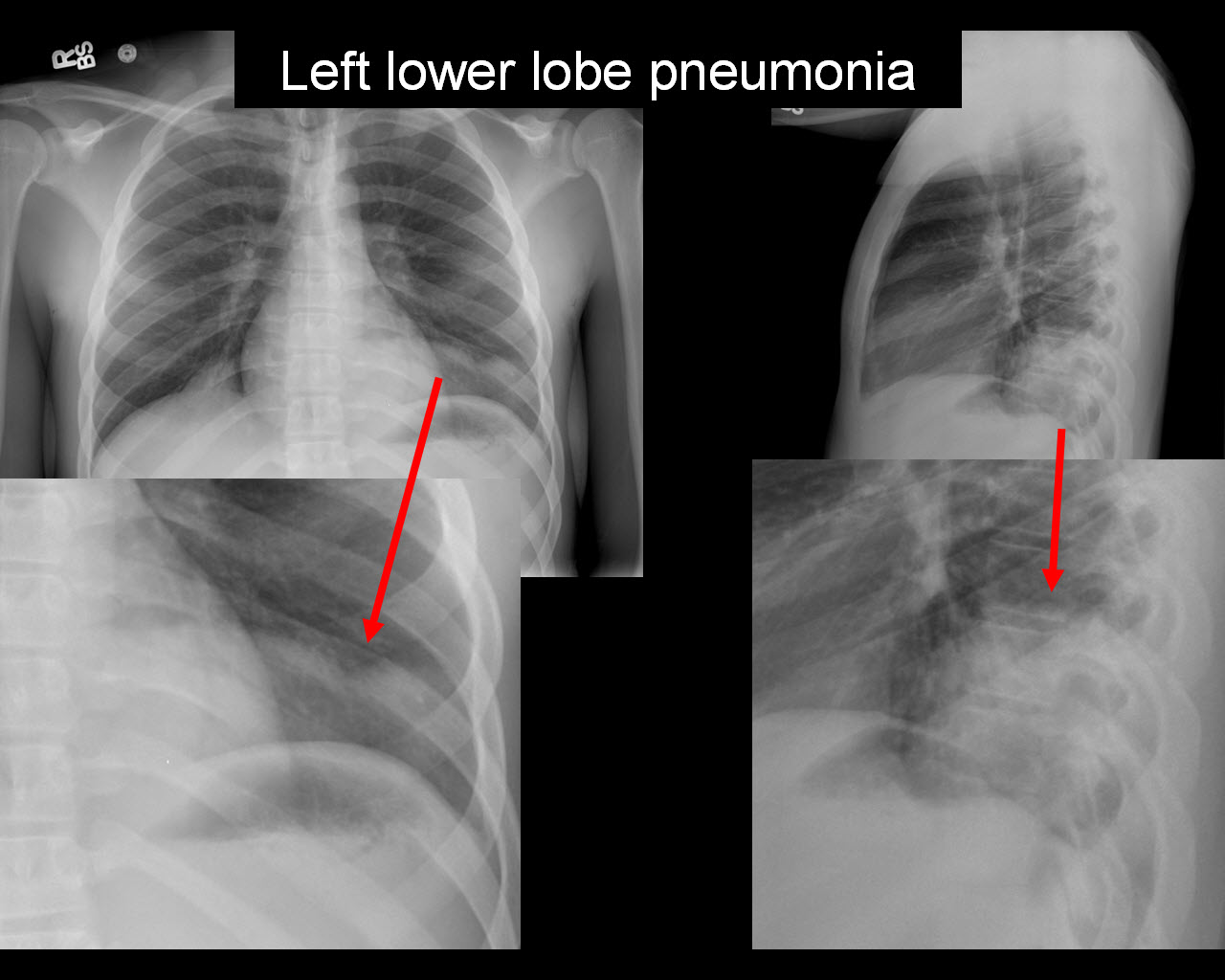
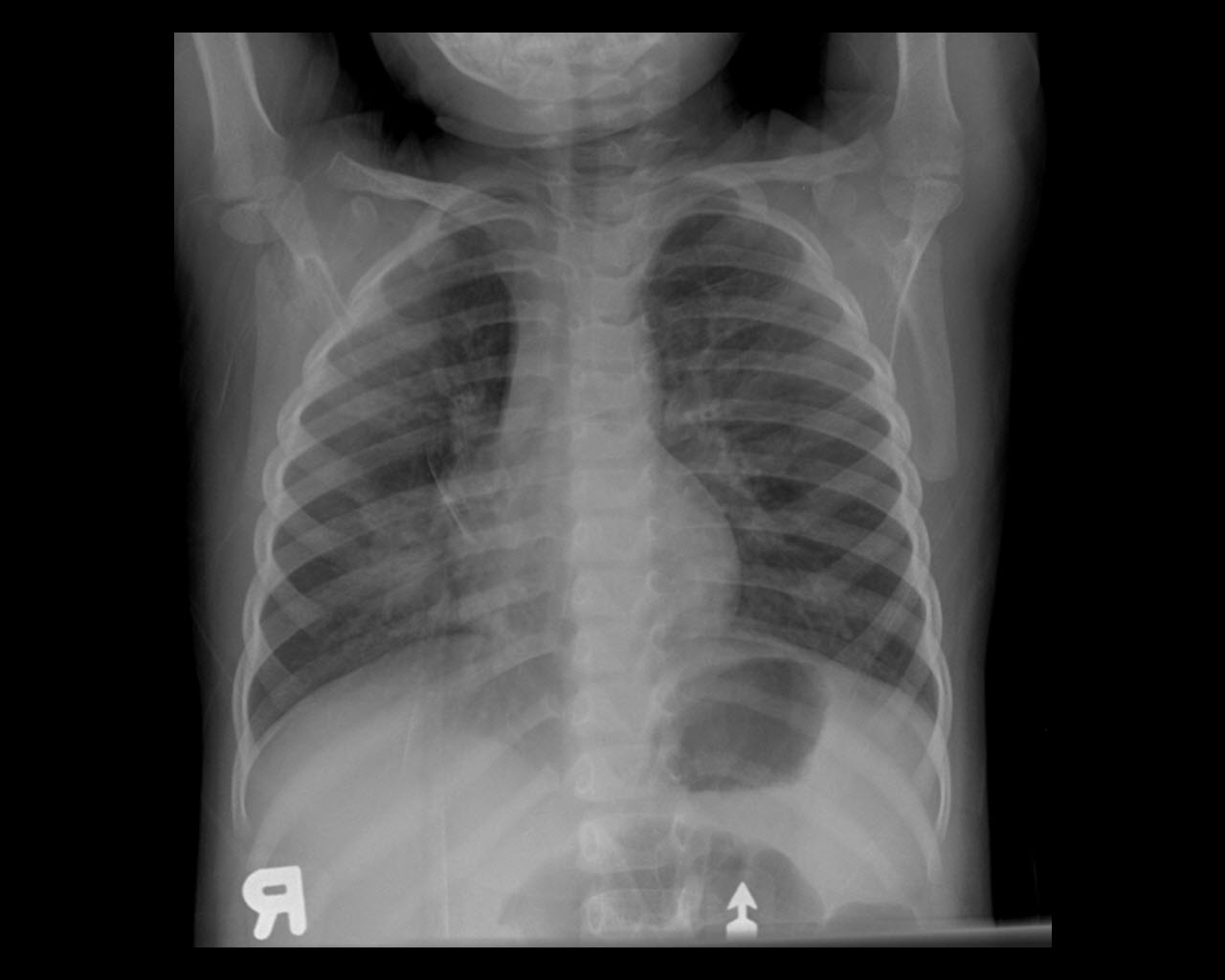
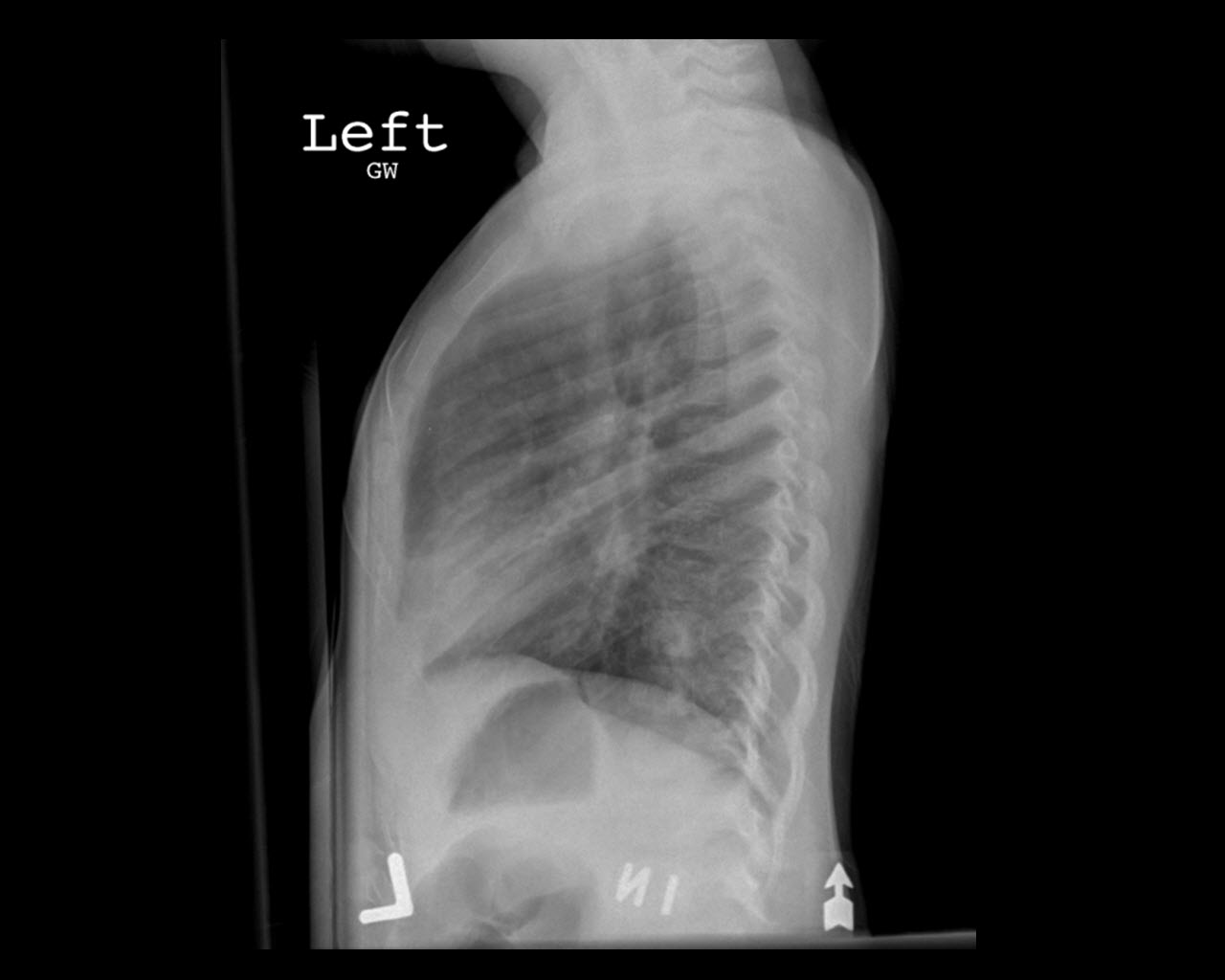
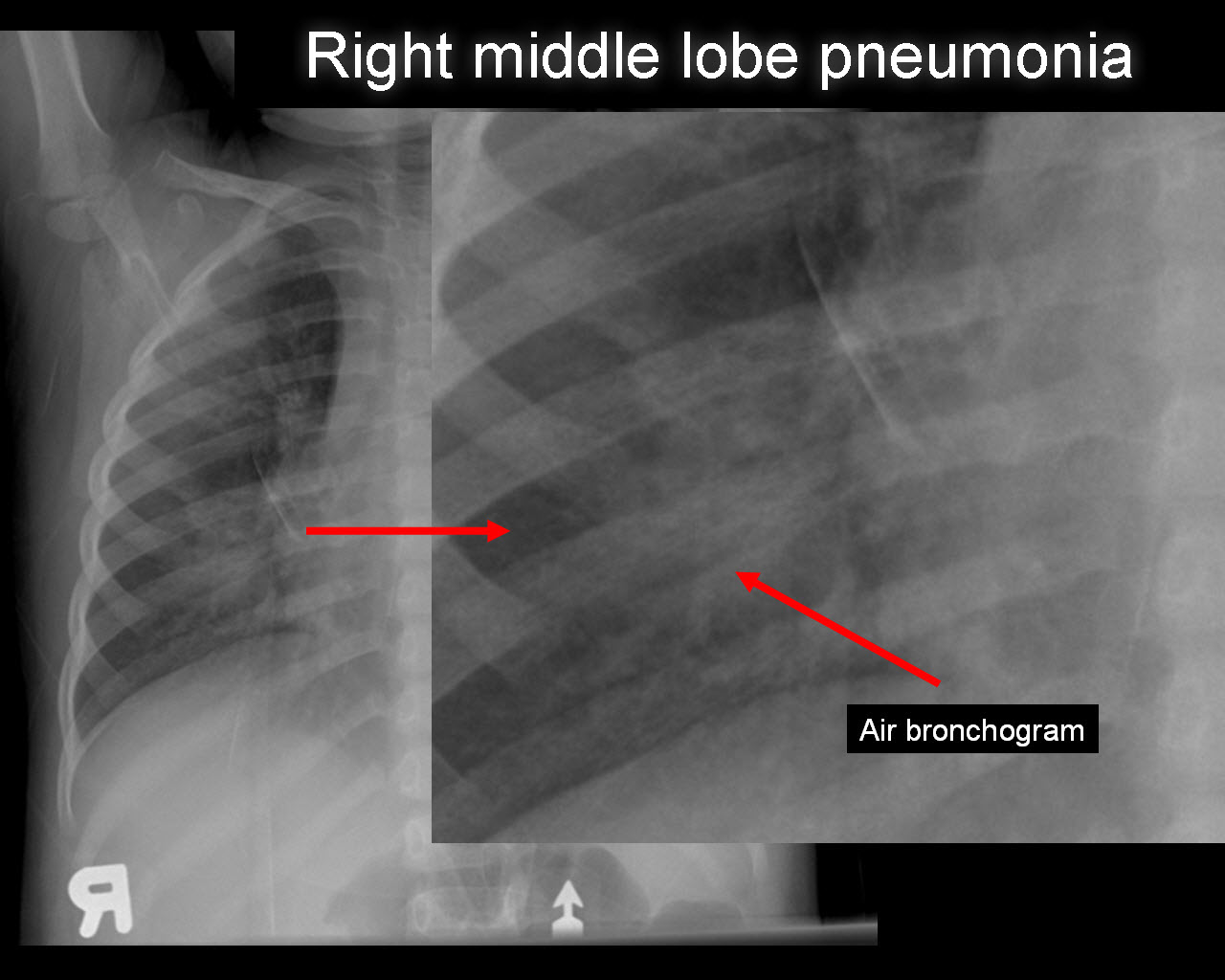
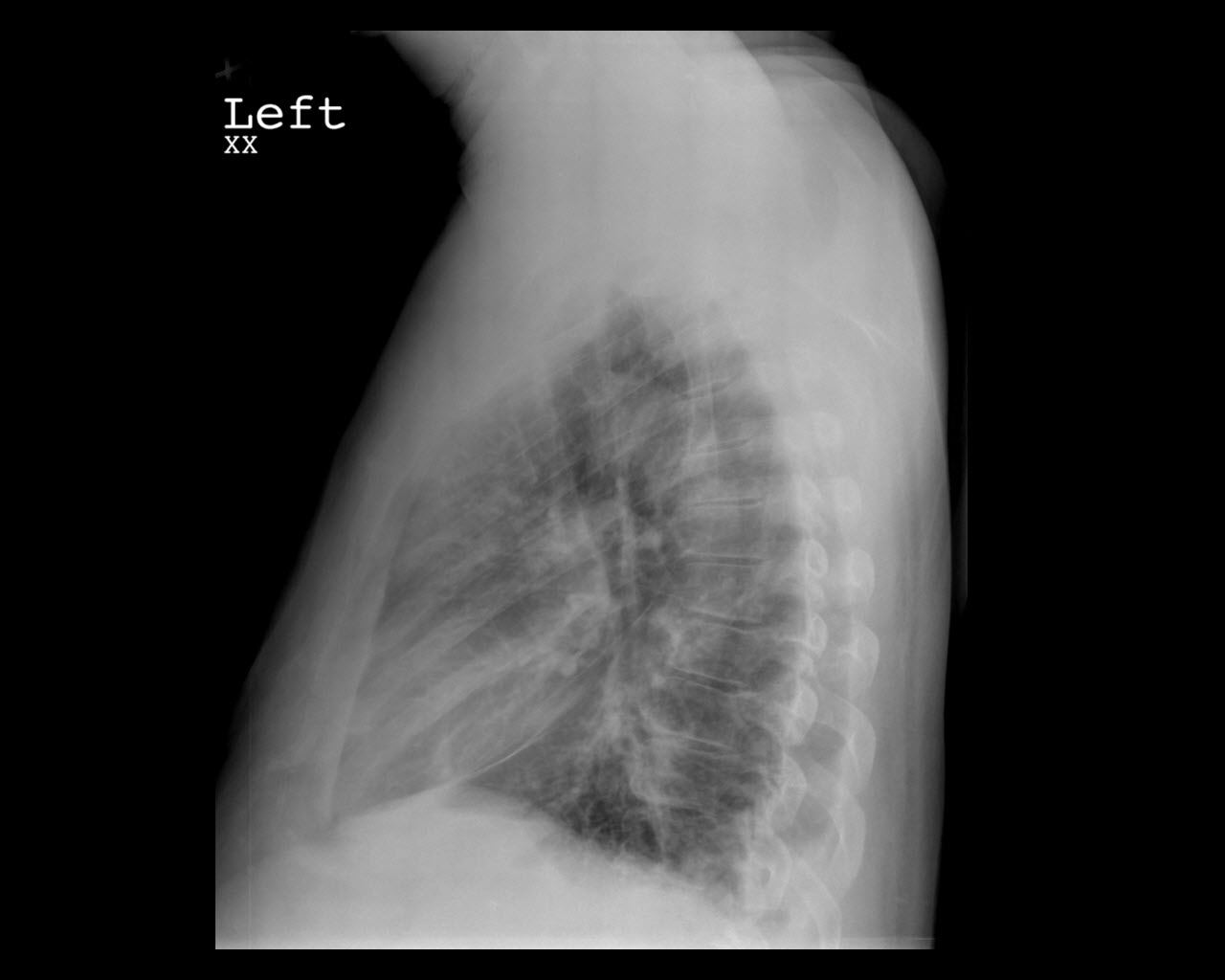
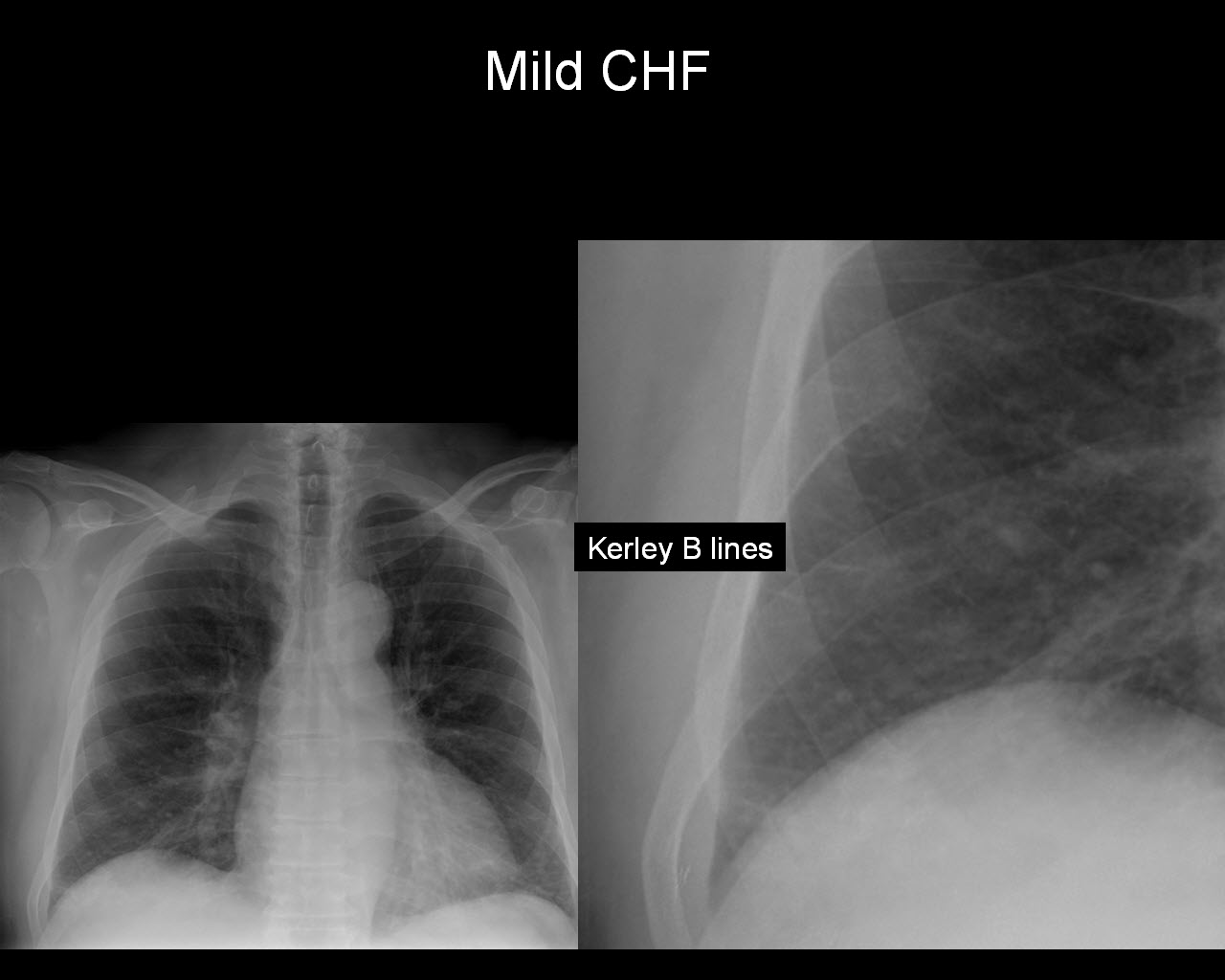
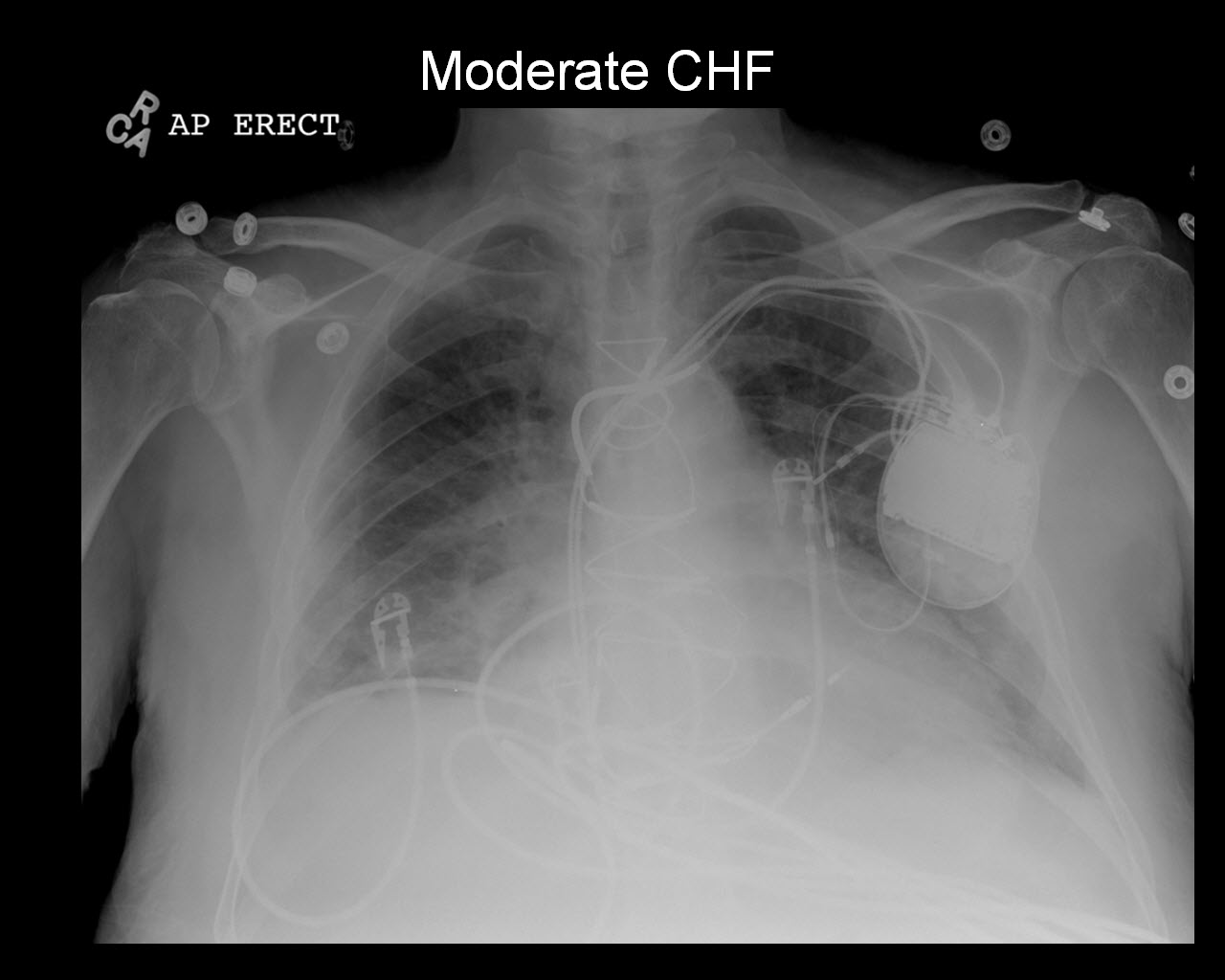
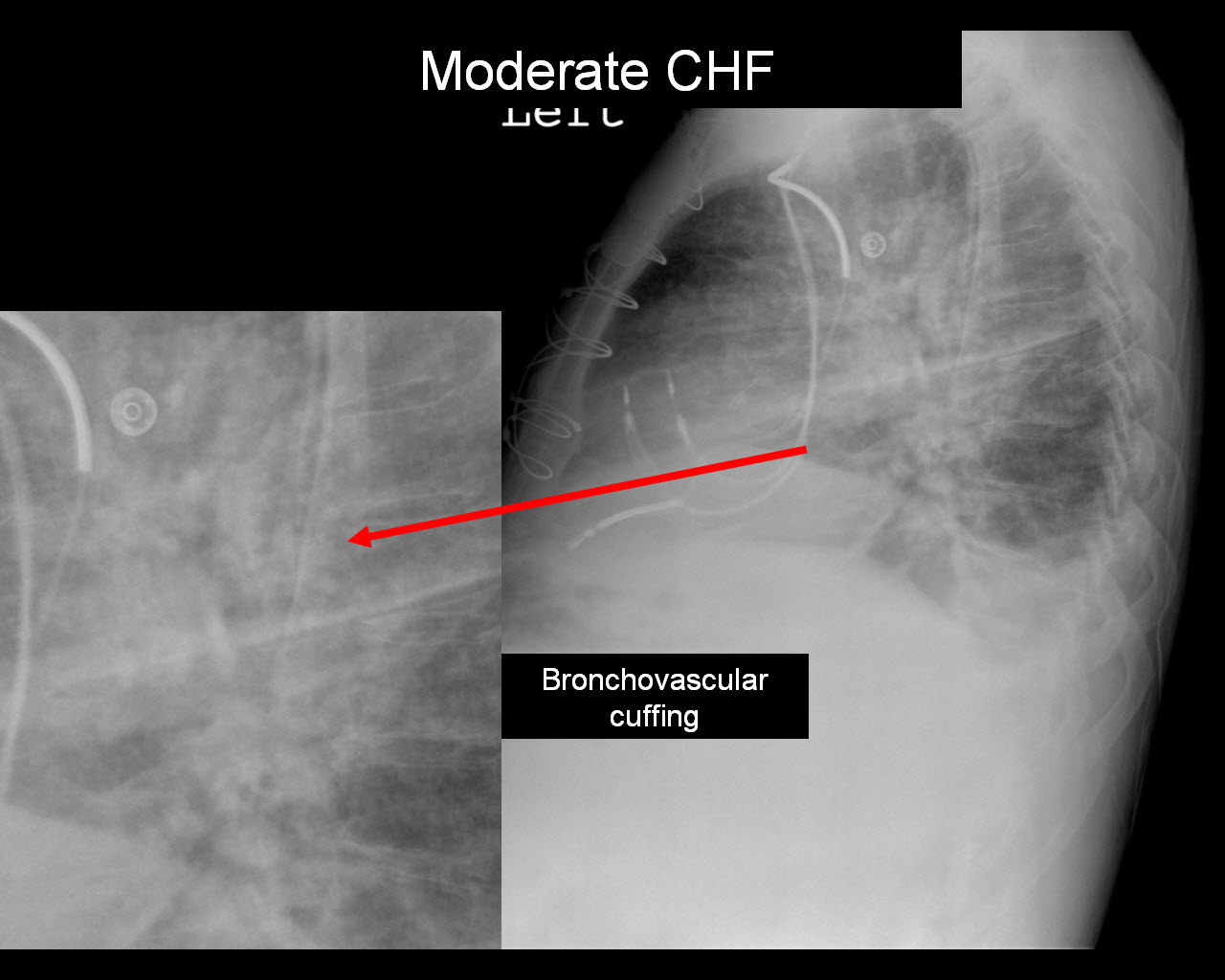
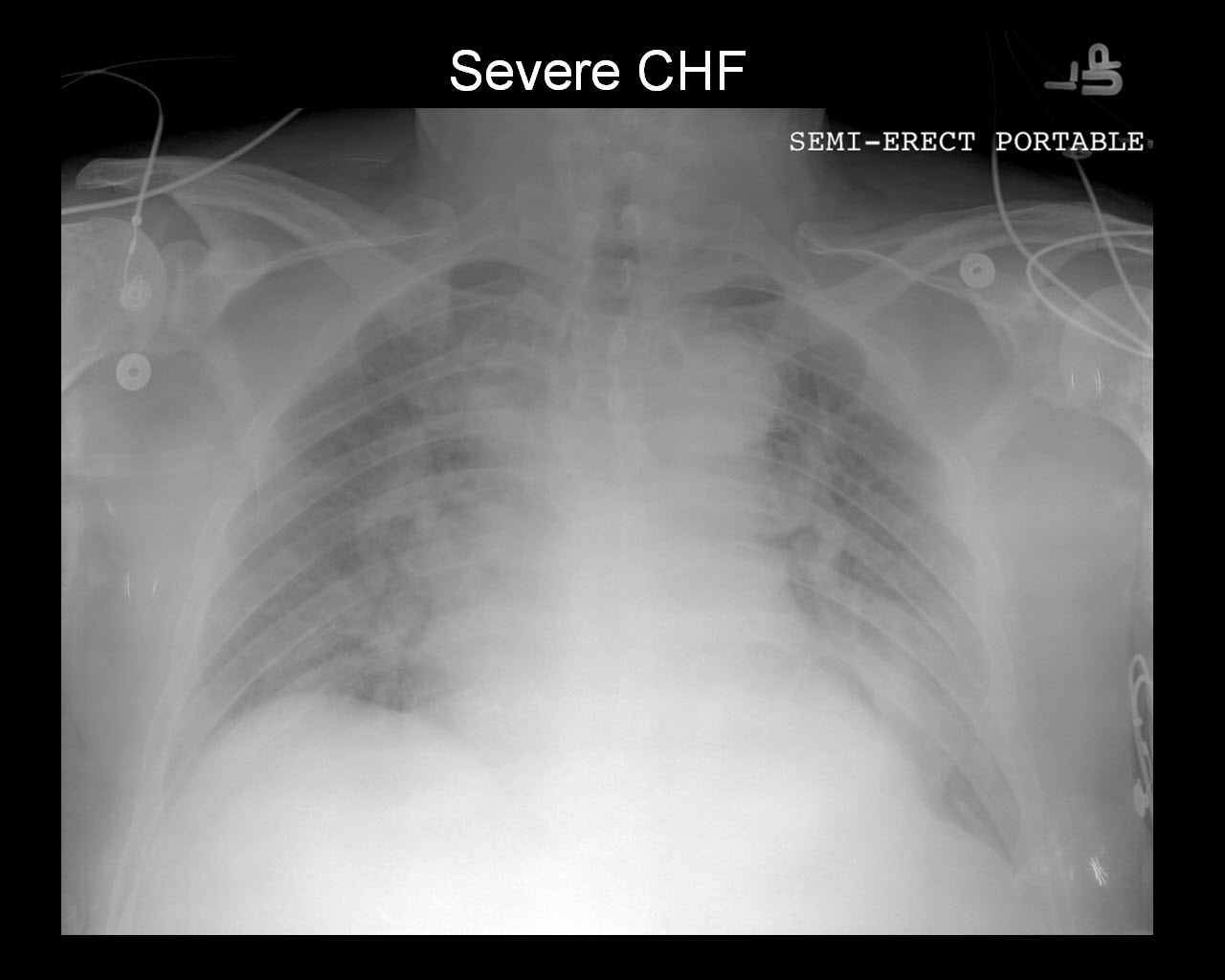
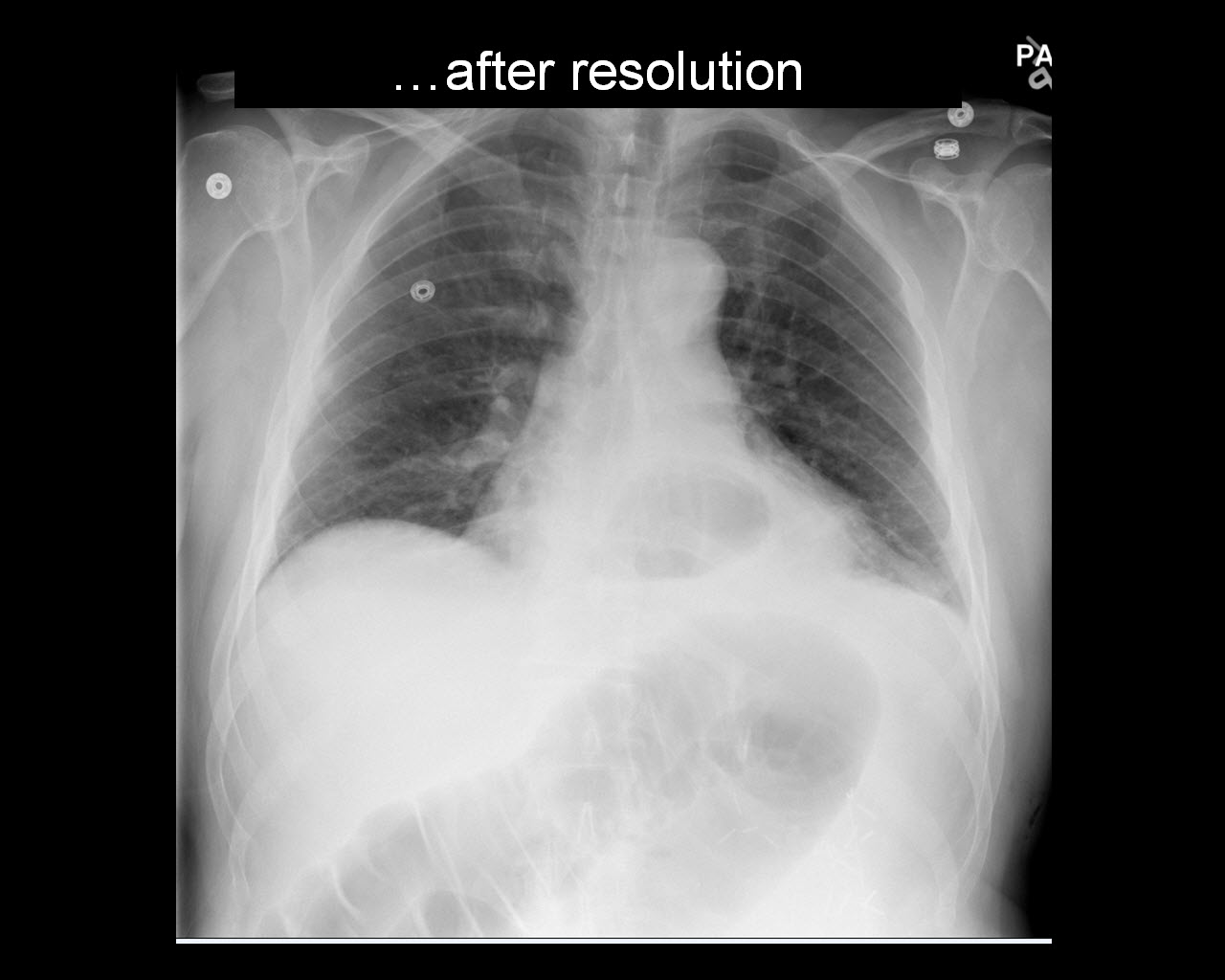
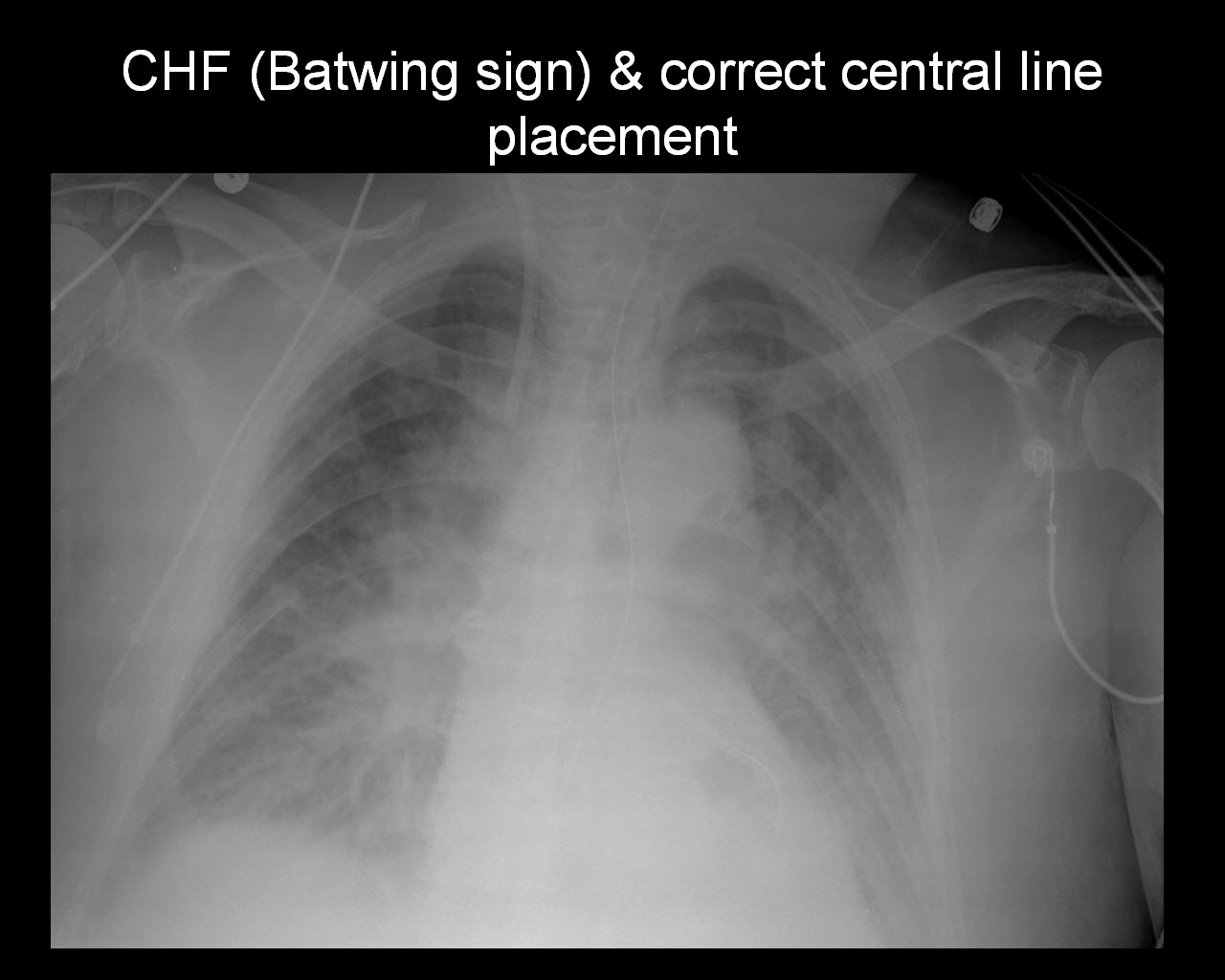
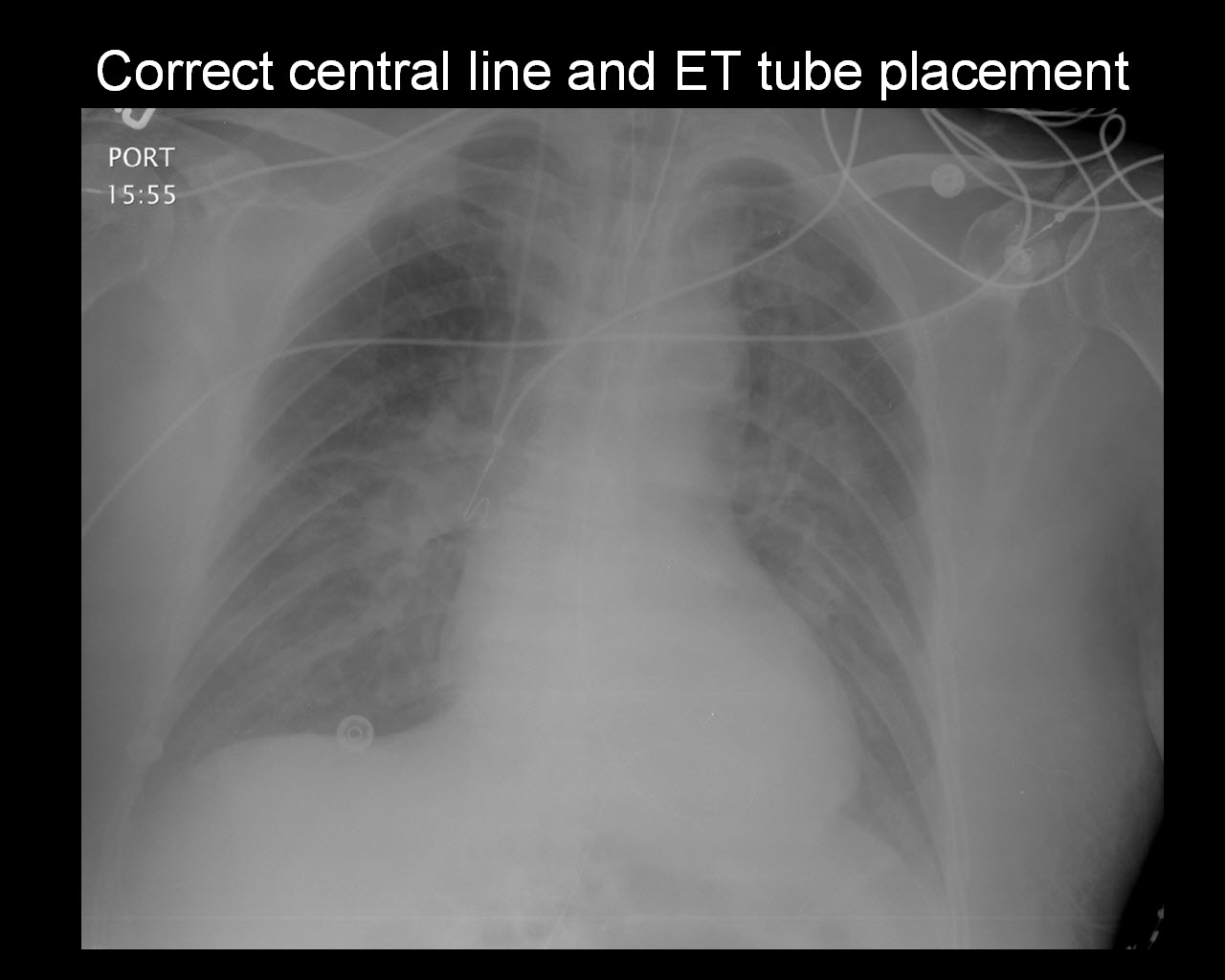
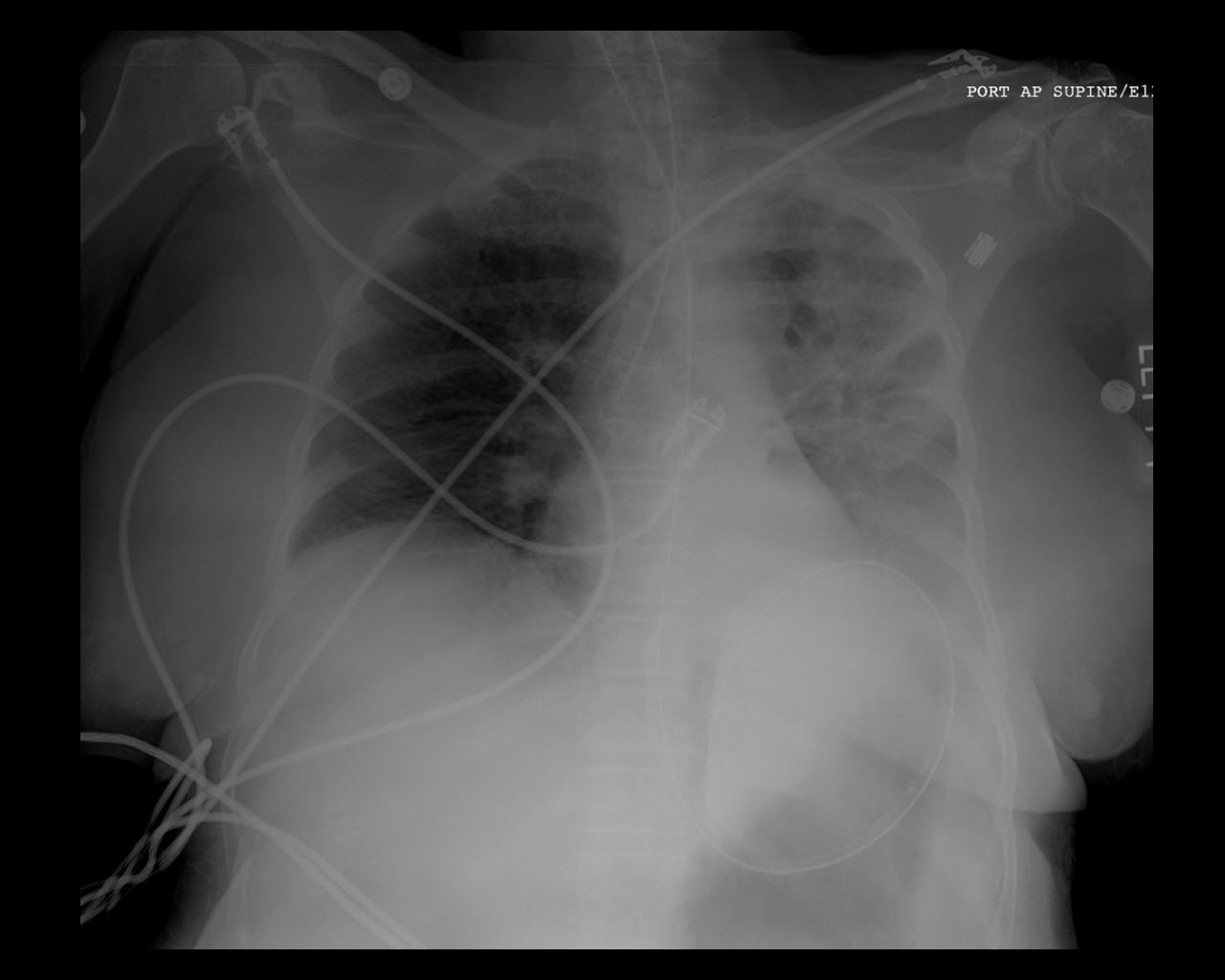
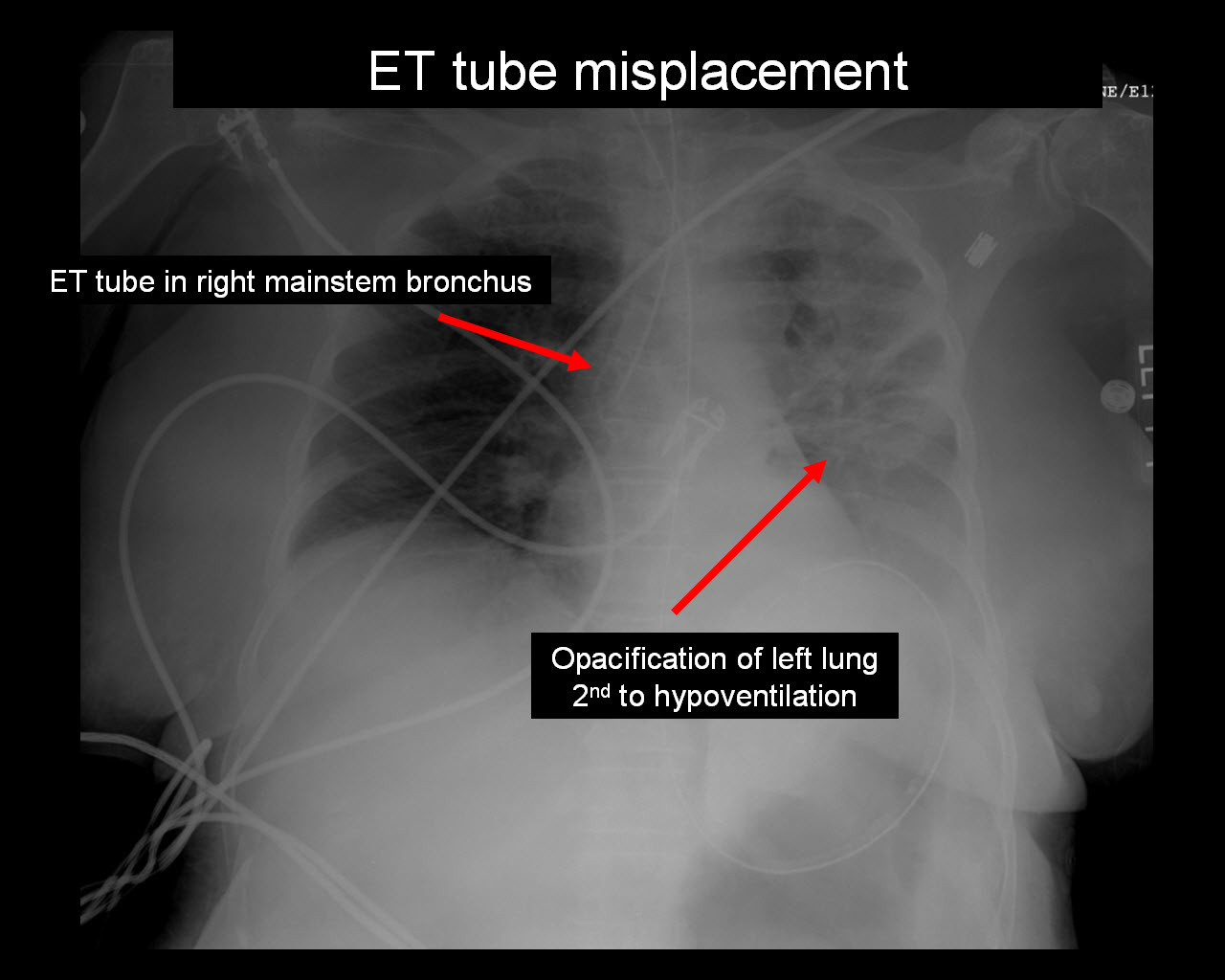
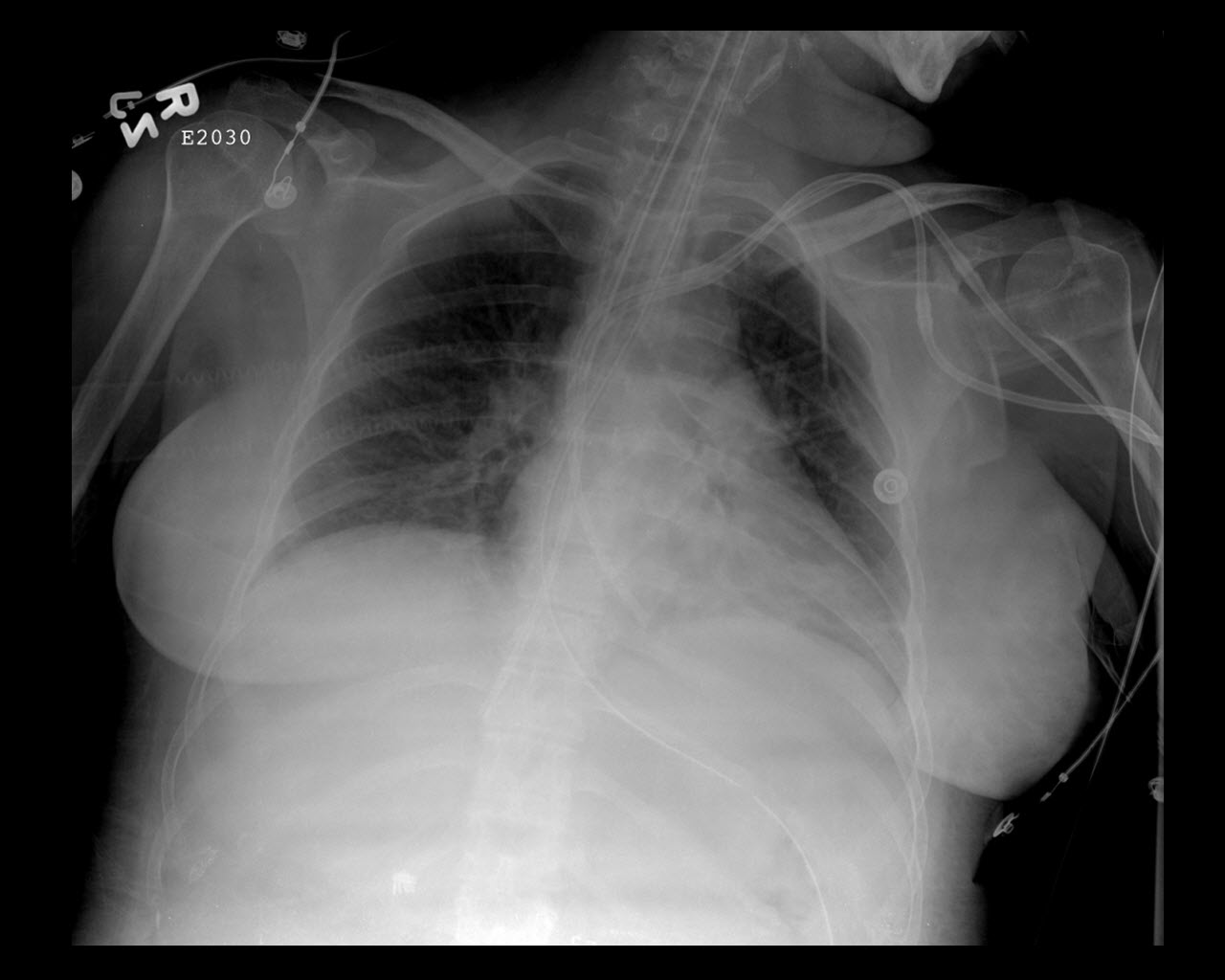
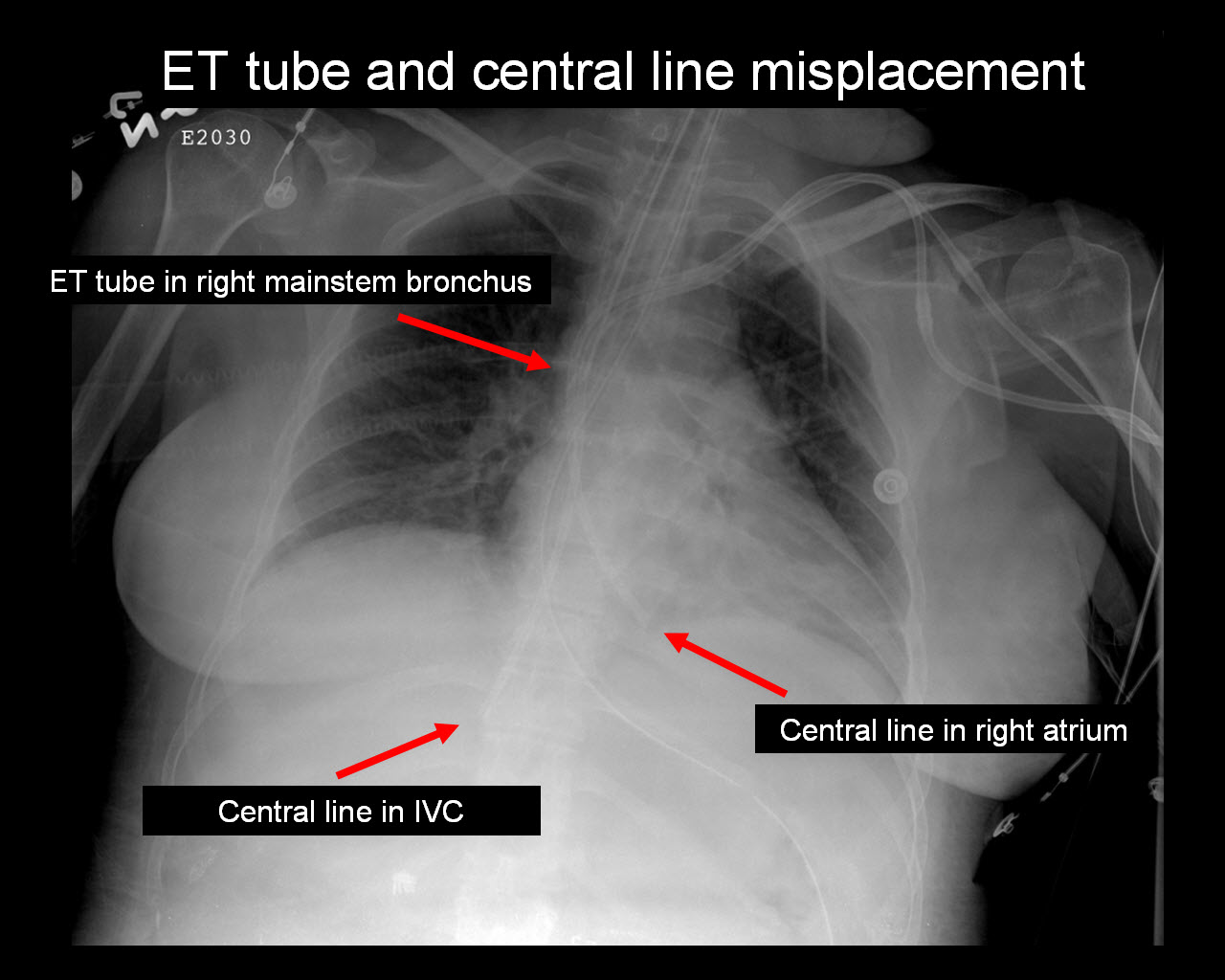
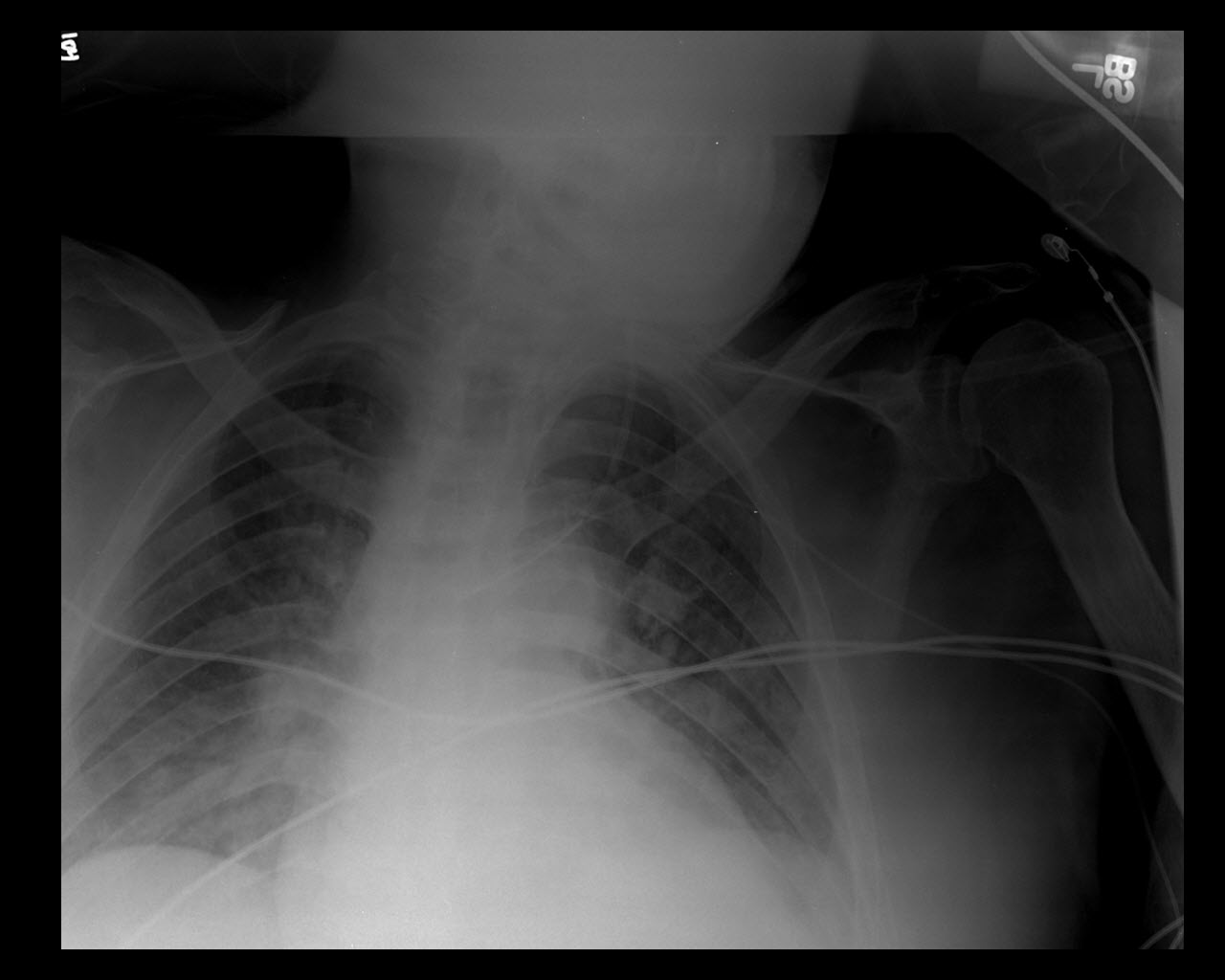
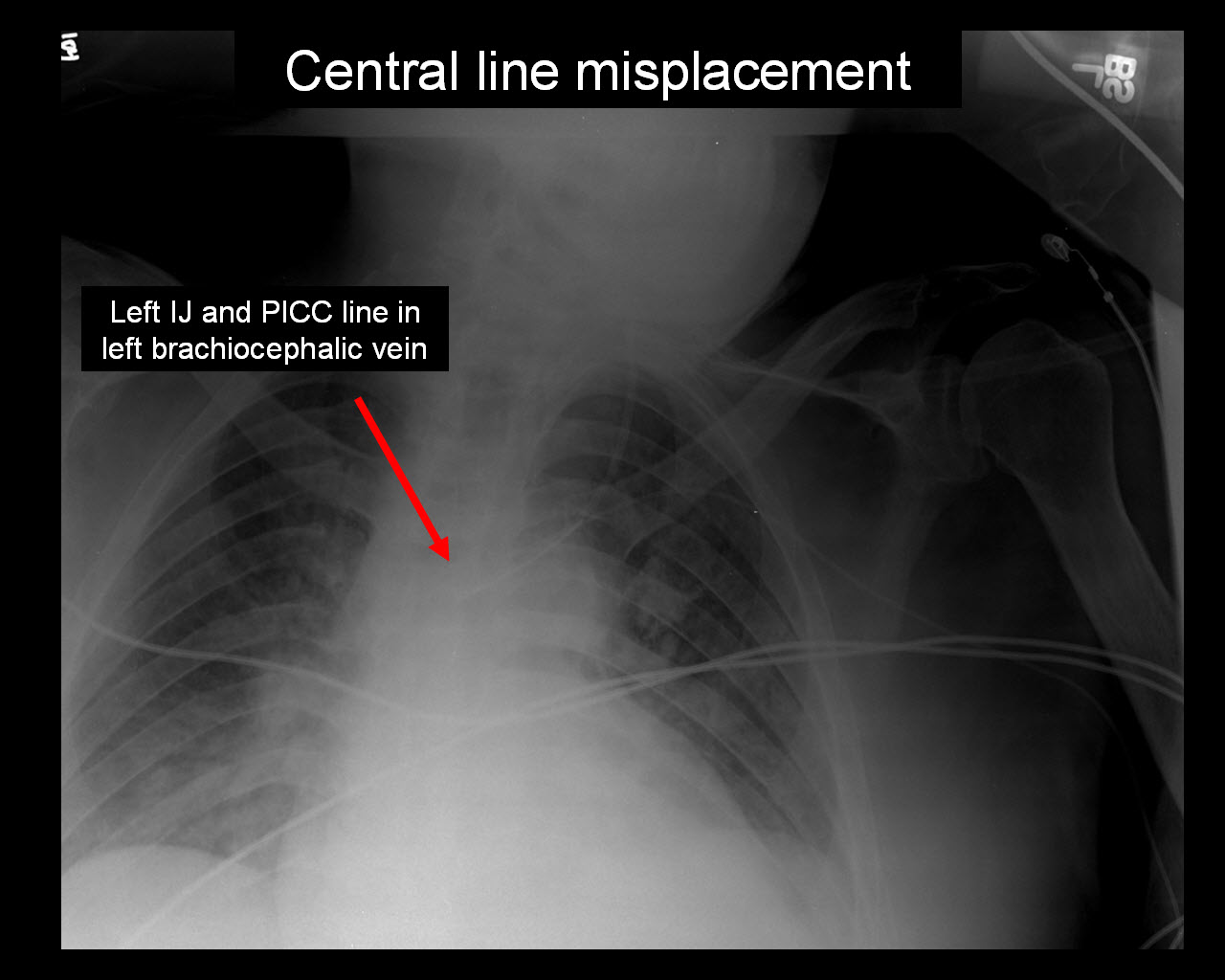
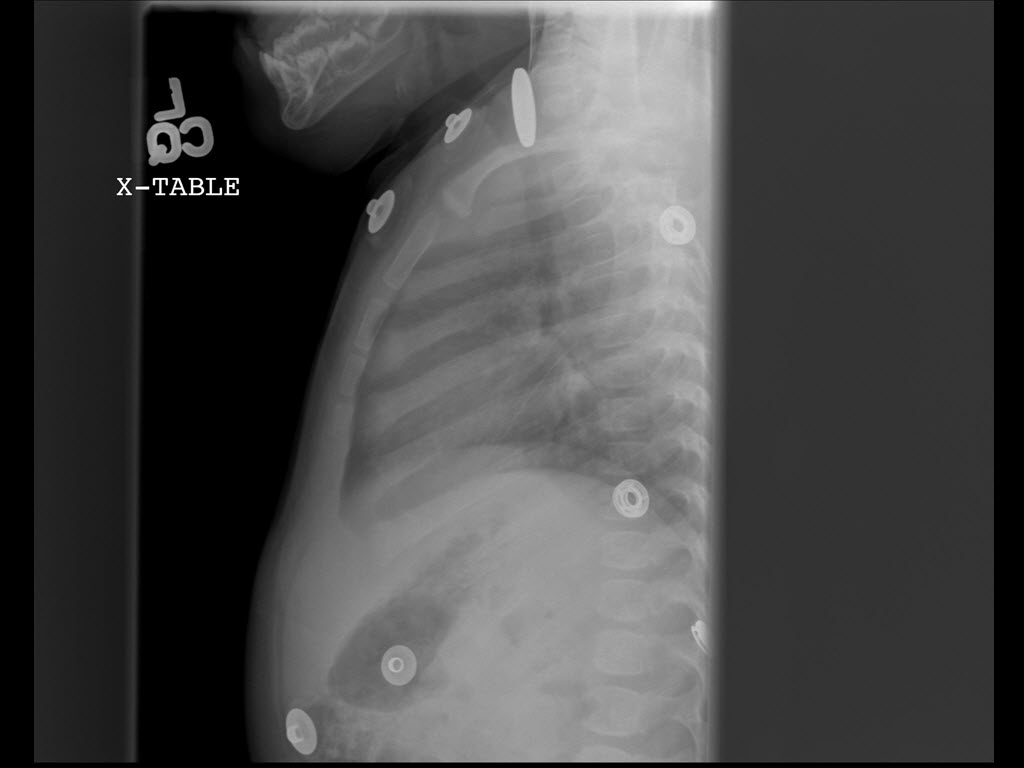
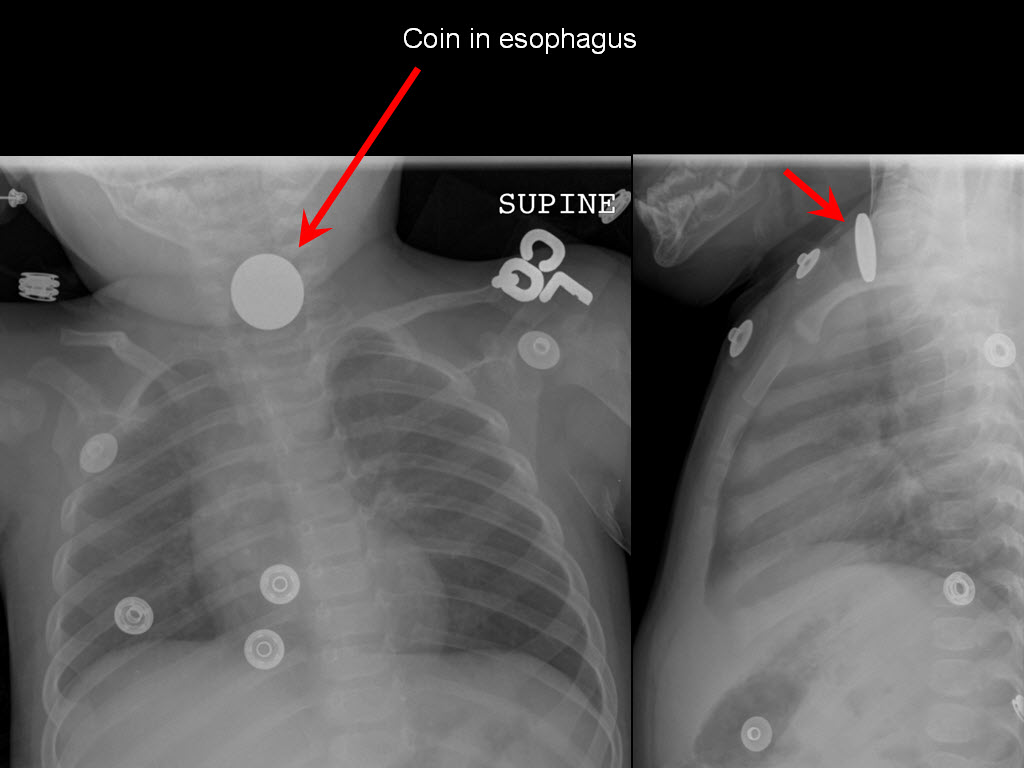
ChestObstructive airways - COPD Thromboembolic disease - Incidental pulmonary embolus on abdominal CT, right atrial thrombus Tube and line misplacement - Misplaced PICC Pneumothorax - Large Pneumothorax Trauma - Serial rib fractures with hemopneumothorax, incidental lung adenocarcinoma Thromboembolic disease - Shower of pulmonary emboli Technique - Normal Chest Harmless - Calcified Granuloma Harmless - Calcified lymph nodes Cancer - Lung cancer Technique - Proper technique important! Pneumothorax - Large pneumothorax Pneumothorax - Small pneumothorax Pneumothorax - Small pneumothorax Pneumothorax - Small costophrenic pneumothorax Aorta - Aortic aneurysm Fluid - Pleural effusion Lung volume - Volume loss Lung volume - Obstructive lung disease Pneumonia - Left and right lower lobe pneumonia Pneumonia - Right middle lobe pneumonia CHF - Mild CHF CHF - Moderate CHF CHF - Severe CHF CHF - Severe CHF (Batwing sign) & correct central line placement Tube and line misplacement - Endotracheal tube and central line placement Tube and line misplacement - ET tube misplacement Tube and line misplacement - ET tube and central line misplacement Tube and line misplacement - Central line misplacement Foreign body - Coin in esophagus Chest: Air where it not belongsDiagnosis: Pneumomediastinum (CT, Radiograph)Air is seen within the subcutaneous soft tissues of neck and chest as well as in the mediastinum - separating mediastinal structures, such as trachea, esophagus and aorta.Chest: Obstructive airwaysDiagnosis: COPD (Radiograph)This patient has hyperinflated lungs: hyperlucent lungs, widened retrosternal space, flattened diaphragms, widened intercostal spaces.Chest: Thromboembolic diseaseDiagnosis: Incidental pulmonary embolus on abdominal CT, right atrial thrombus (CT)This pulmonary embolus has a more chronic appearance, since it is more wall adherend. Acute emboli are more centrally located within the vessel. Also right atrial thrombus.Chest: Tube and line misplacementDiagnosis: Misplaced PICC (Plain film, Radiograph)A right PICC has a somewhat serpiginous course with the tip projecting over the right lower neck. Also noted is a moderate right pleural effusion.Chest: PneumothoraxDiagnosis: Large Pneumothorax (Plain film, Radiograph)A single AP upright view of chest shows advanced left pneumothorax with associated advanced collapse of left lung.Chest: TraumaDiagnosis: Serial rib fractures with hemopneumothorax, incidental lung adenocarcinoma (CT)CT in soft tissue, bone and lung windows demonstrate acute fractures of the right sixth through ninth ribs laterally and posterolaterally and a tiny right hemopneumothorax.Chest: Thromboembolic diseaseDiagnosis: Shower of pulmonary emboli (CT)Multiple luminal filling defects are seen in the segmental and subsegmental branches of bilateral pulmonary arteries, consistent with a shower of acute pulmonary emboli. The more central luminal location of the emboli speaks more for an acute event.Chest: TechniqueDiagnosis: Normal Chest (Plain film, Radiograph)Proper technique important: Chest: HarmlessDiagnosis: Calcified Granuloma (Plain film, Radiograph)Dense calcificationWell defined Sharp margins Size < 1cm Chest: HarmlessDiagnosis: Calcified lymph nodes (Plain film, Radiograph, CT, Computed tomography)Calcified lymph nodes (from histoplasmosis)(Bi)hilar calcifictions Sometimes �lymph node� shaped History helpful (Histoplasmosis, Sarcoidosis, Tuberculosis, etc.) Chest: CancerDiagnosis: Lung cancer (Plain film, Radiograph)Poorly (if not) calcifiedWell � poor margins Size > 1cm History (smoker, Asbestos exposure) Here: RLL tumor (SCC) Chest: TechniqueDiagnosis: Proper technique important! (Plain film, Radiograph)Importance of good inspiration and erect techniquePortable (AP) films: Lungs underairated (mimicking, tumors or infiltrates) Heart larger Chest: PneumothoraxDiagnosis: Large pneumothorax (Plain film, Radiograph)Look along the pleural margins!No vascular markings beyond pleural line Ipsilateral lung collapsed/ more dense (depends on size) Can hide behind ribs History (central line placement, emphysema, trauma, tumor) Look for tension pneumothorax (mediastinal shift away from pneumo) Chest: PneumothoraxDiagnosis: Small pneumothorax (Plain film, Radiograph)Look along the pleural margins!No vascular markings beyond pleural line Ipsilateral lung collapsed/ more dense (depends on size) Can hide behind ribs History (central line placement, emphysema, trauma, tumor) Look for tension pneumothorax (mediastinal shift away from pneumo) Chest: PneumothoraxDiagnosis: Small pneumothorax (Plain film, Radiograph)Look along the pleural margins!No vascular markings beyond pleural line Ipsilateral lung collapsed/ more dense (depends on size) Can hide behind ribs History (central line placement, emphysema, trauma, tumor) Look for tension pneumothorax (mediastinal shift away from pneumo) Chest: PneumothoraxDiagnosis: Small costophrenic pneumothorax (Plain film, Radiograph)Look along the pleural margins!No vascular markings beyond pleural line Ipsilateral lung collapsed/ more dense (depends on size) Can hide behind ribs History (central line placement, emphysema, trauma, tumor) Look for tension pneumothorax (mediastinal shift away from pneumo) Chest: AortaDiagnosis: Aortic aneurysm (Plain film, Radiograph, CT, Computed tomography)Thoracic aortic aneurysmProminence of aortic arch and/or descending aorta Chest: FluidDiagnosis: Pleural effusion (Plain film, Radiograph, CT, Computed tomography)Small (blunting of costophrenic angle) toLarge (partial/complete opacification of the lung) Multiple etiologies (CHF, trauma, postoperative, malignant, infectious) If unsure, do decubitus view (fluid moves � solid lesions don�t!) Here: Large pleural effusion Chest: Lung volumeDiagnosis: Volume loss (Plain film, Radiograph)Multiple etiologies (surgical, atelectasis, pneumothorax) Mediastinal shift towards the lesion (traction) Compared to space occupying lesions: Mediastinal shift away from lesion (mass effect)Here: Status post left pneumonectomy Chest: Lung volumeDiagnosis: Obstructive lung disease (Plain film, Radiograph)Etiologies: COPD, Asthma etc.Hyperinflated lungs Flat diaphragms Wide intercostal spaces Horizontal oriented ribs Wide retrosternal space �Relatively� small heart Chest: PneumoniaDiagnosis: Left and right lower lobe pneumonia (Plain film, Radiograph)Lung infiltrateAir bronchogram Physical correlation important (fever, leucocytosis, cough) Lower lungs (right > left) likely due to aspiration Chest: PneumoniaDiagnosis: Right middle lobe pneumonia (Plain film, Radiograph)Lung infiltrateAir bronchogram Physical correlation important (fever, leucocytosis, cough) Lower lungs (right > left) likely due to aspiration Chest: CHFDiagnosis: Mild CHF (Plain film, Radiograph)Enlarged heartProminent central vessels Kerley B lines Patchy lung opacifications Cephalization (upper vessels prominent) Chest: CHFDiagnosis: Moderate CHF (Plain film, Radiograph)Enlarged heartProminent central vessels Kerley B lines Patchy lung opacifications Cephalization (upper vessels prominent) Chest: CHFDiagnosis: Severe CHF (Plain film, Radiograph)Enlarged heartProminent central vessels Kerley B lines Patchy lung opacifications Cephalization (upper vessels prominent) Chest: CHFDiagnosis: Severe CHF (Batwing sign) & correct central line placement (Plain film, Radiograph)Enlarged heartProminent central vessels Kerley B lines Patchy lung opacifications Cephalization (upper vessels prominent) Chest: Tube and line misplacementDiagnosis: Endotracheal tube and central line placement (Plain film, Radiograph)ET tube tip between sternoclavicular joint and carinaCentral line tip between proximal and distal SVC Chest: Tube and line misplacementDiagnosis: ET tube misplacement (Plain film, Radiograph)ET tube in right mainstem bronchusOpacification of left lung 2nd to hypoventilation Chest: Tube and line misplacementDiagnosis: ET tube and central line misplacement (Plain film, Radiograph)ET tube in right mainstem bronchusCentral line in right atrium Central line in IVC Chest: Tube and line misplacementDiagnosis: Central line misplacement (Plain film, Radiograph)Left IJ and PICC line in left brachiocephalic veinChest: Foreign bodyDiagnosis: Coin in esophagus (Plain film, Radiograph)Don't be confused by all the other lead buttons! There is a coin shaped foreign body projecting over the lower neck. On the lateral view it projects over the esophagus/trachea. However, it HAS to be in the esophagus, because it is en face on the PA view. If it would be in the trachea it would be en face on the lateral vie. The reason is, that the posterior wall of the trachea is membranous and has the least resistance, allowing the esophagus to orient in a AP position. Once again: en face on the PA view: in the esophagus - en face on the lateral view: in the trachea.Home :: Contact Us Make On Call Radiology your homepage :: Add On Call Radiology to your favorites |